* Do not miss the test on this topic on the TEST PACKAGES page.
This blog prepares you for
GPAT
D.Pharm, B.Pharm, and Pharm.D. Exams
RRB Pharmacist Recruitment Exam
Common Recruitment Examination for AIIMS Pharmacist
KGMU Pharmacist Recruitment Exam
KSSSCI Pharmacist Recruitment Exam
MPESB Pharmacist Recruitment Exam
Drugs Inspector Exams
Drugs Controller Exams
DPEE
• Adrenaline and noradrenaline are also known as epinephrine and norepinephrine respectively.
• Adrenaline and noradrenaline are hormones and neurotransmitters produced by the adrenal glands and adrenergic nerve endings.
• As a neurotransmitter, adrenaline and noradrenaline are involved in sympathetic nervous system.
• Adrenaline and noradrenaline are direct acting sympathomimetic agents. They bind to and activate adrenergic receptors directly.
• Adrenaline has α1, α2, β1, β2 and weak β3 action.
• Noradrenaline has α1, α2, β1, β3 but no β2 action.
• Tyrosine is considered to be the precursor for the biosynthesis of noradrenaline.
• The enzyme involved in the conversion of noradrenaline to adrenaline is N-methyltransferase.
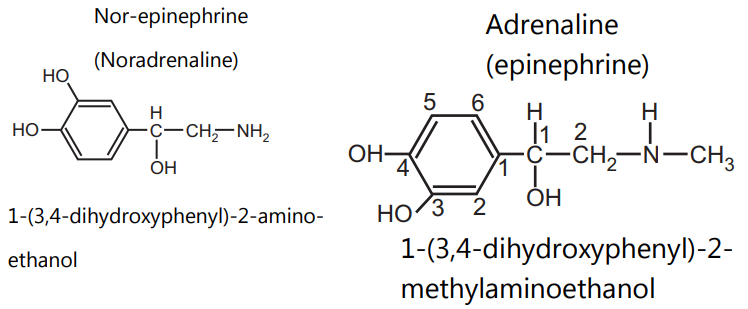
• Adrenaline and noradrenaline are catecholamines.
• The structural difference between adrenaline and noradrenaline is the presence of an N-methyl group in adrenaline, which is absent in noradrenaline. (See structures)
• Noradrenaline is a white or brownish white crystalline powder, soluble in water.
• Adrenaline is a white microcrystalline powder, soluble in water.
Pharmacological Actions of Adrenaline
• Heart: Adrenaline with its action on β1-receptors of heart increases heart rate (positive chronotropic), force of contraction (positive inotropic), conduction velocity (positive dromotropic) and cardiac output. It may produce ventricular arrhythmia.
• Blood Vessels: Both vasoconstriction (through α1 receptor) and vasodilatation (through β2 receptor) can occur depending on the dose and the vascular bed. Vasoconstriction occurs peripherally in skin, mucous membrane and renal beds. Vasodilatation predominates in skeletal muscles, liver and coronaries.
• Blood Pressure: Adrenaline by slow IV infusion or SC injection causes rise in systolic BP (by myocardial action) but fall in diastolic BP. The reason for this fall in diastolic BP is more sensitivity of vascular β2 receptors than α1 receptors.
In animals, rapid IV injection of adrenaline produces biphasic response. Initially, it causes peripheral vasoconstriction and leads to rise in systolic BP. This is followed by dilation of skeletal muscle blood vessels, decrease in resistance and output, and fall in diastolic BP. This response of adrenaline is known as biphasic response.
Dales vasomotor reversal: If vasoconstriction action of adrenaline is blocked by α1 blocker, it causes only fall in BP. This reversal of action of adrenaline from biphasic to monophasic response on blood pressure is called as Dales vasomotor reversal.
• Smooth Muscles: Adrenaline relaxes smooth muscles due to action on β2 receptors. It is a powerful bronchodilator.
• Central Nervous System: In clinically used doses adrenaline may produce tremors, restlessness, palpitation and apprehension.
• Eye: Topical application of adrenaline may cause mydriasis and fall in intraocular tension.
• Metabolism:
(i) Adrenaline causes glycogenolysis leading to hyperglycaemia and hyperlactacidaemia.
(ii) It also causes lipolysis which leads to increase in plasma free fatty acid (FFA) and calorigenesis (β2 + β3).
(iii) In addition metabolic effects result from reduction of insulin and augmentation of glucagon secretion.
• Antiallergic Actions: Adrenaline is a physiological antagonist of histamine and counters the bronchoconstriction and hypotension of anaphylactic shock.
• Adrenaline is orally inactive because it is rapidly degraded by monoamine oxidase (MAO) and catechol O methyl transferase (COMT) present in the intestinal wall and liver.
• MAO causes the intraneuronal metabolism of catecholamines and COMT causes extraneuronal metabolism of catecholamines.
• Adrenaline can treat a number of life threatening medical emergencies such as anaphylactic shock, asthma and bronchospasm, cardiac shock, severe upper airway obstruction, uncontrolled bleeding, etc.
• Its peripheral vasoconstrictor property can be used to stop nasal and dental bleeding.
• Adrenaline is given along with local anaesthetics to produce local anaesthesia because adrenaline causes peripheral vasoconstriction resulting in (i) decreased systemic absorption of local anesthetics, (ii) prolonged duration of action of local anesthetics, (iii) decreased dose of local anaesthetics and (iv) decreased systemic toxicity of local anaesthetics.
• Adrenaline with local anaesthetics is a synergistic combination.
• Noradrenaline (Norepinephrine, levarterenol): Noradrenaline causes rise in systolic, diastolic and mean BP. It increases peripheral resistance consistently due to α action. It doesn’t have β2 action (vasodilation). It is a drug of choice for acute hypotensive shock.
• Hypertension, hyperthyroid, angina patients, occlusive vascular disease, hypersensitivity, cardiac arrhythmias or tachycardia, angle-closure glaucoma (eye drops) are some of the contraindications for adrenaline.
SAR of Phenylethanolamine Adrenergic Agonists (See structures)
Adrenaline and noradrenaline are phenylethanolamine.
In phenylethanolamine adrenergic agonists, a primary or secondary aliphatic amine separated by two carbons from a substituted benzene ring is minimally required for high agonist activity. These agents also have a hydroxyl group on C1 of the side chain, β to the amine, as in adrenaline and noradrenaline.
Stability and Storage Conditions of Adrenaline
• Adrenaline can be oxidized by air or oxygen to get pink or red colour complex.
• It darkens on exposure to light and air.
• It is stored in tightly closed light resistant containers.
MCQs
1. Identify the incorrect statement: Adrenaline is added to local anaesthetics to _____.
a) enhance bioavailability of local anaesthetics
b) prolong the duration of action of local anaesthetics
c) reduce the systemic absorption of local anaesthetics
d) reduce systemic toxicity of local anaesthetics
2. Secondary amine is a part of___
a) Adrenaline
b) Noradrenaline
c) Dopamine
To proceed with the TEST ON ADRENALINE & NORADRENALINE,
Click here
Blog content and MCQs have been taken from the following:
1) Essential Pharmacy Review for Drugs Inspector Exams by Nirali Prakashan, Pune
To know more about the book:
Click here
2) Pharmacist Recruitment Exam by Nirali Prakashan, Pune
To know more about the book:
Click here
To know more about our DPEE book DIPLOMA IN PHARMACY EXIT EXAMINATION (DPEE) – Based on PCI-ER 2020 Syllabus (5000+ MCQs)
Click here
PHARMACOLOGY (Second Year Diploma in Pharmacy PCI – ER 2020)
Authors: Sunil R. Bakliwal , Praneta R. Desale , Pravin P. Jawale
This book includes more than 500 MCQs for the preparation of DPEE and various Pharmacist Recruitment Exams
To know more about the book:
Click here