Assam Rifles Pharmacist Recruitment 2025
Are you preparing for the CRE-AIIMS Pharmacist Exam? As the exam approaches, it Is crucial to make sure you are fully prepared with the right resources and study tools. At this stage of your exam prep, a final review can make all the difference between success and a missed opportunity. CRE-AIIMS Pharmacist Exam Schedule Date of Examination: 26th February 2025 Shift of Examination: Evening Shift Check official website given below.
राजस्थान कर्मचारी चयन बोर्ड, जयपुर ने राष्ट्रीय स्वास्थ्य मिशन और राजस्थान मेडिकल एज्यूकेशन सोसायटी के संविदा पदों के लिए ऑनलाइन आवेदन प्रक्रिया की तिथि में संशोधन किया है। विज्ञप्ति संख्या 01/2025 दिनांक 28 जनवरी 2025 के अनुसार, पहले ऑनलाइन आवेदन 18 फरवरी 2025 से 19 मार्च 2025 तक किए जाने थे, लेकिन तकनीकी कारणों के चलते आवेदन की तिथि में बदलाव किया गया है। अब उम्मीदवार 19 मार्च 2025 से लेकर 17 अप्रैल 2025 रात 11:59 बजे तक ऑनलाइन आवेदन और पंजीयन शुल्क जमा कर सकते हैं। कर्मचारी चयन बोर्ड ने आवेदकों को सलाह दी है कि वे अंतिम तिथि का इंतजार किए बिना समय सीमा के भीतर आवेदन प्रक्रिया पूरी करें। इस संशोधित विज्ञप्ति में बाकी सभी शर्तें पूर्व में जारी विज्ञप्ति के अनुसार ही रहेंगी। अधिक जानकारी के लिए उम्मीदवार बोर्ड की आधिकारिक वेबसाइट पर विजिट करें।

Notification No.04/MRB/2025 Dated:17.02.2025. 1. Applications are invited only through online mode up to 10.03.2025 for direct recruitment on temporary basis to the post of Pharmacist in Tamil Nadu Medical Subordinate Service. 2. No. of vacancies: 425 Date of Notification 17.02.2025 Last date for submission of Application: 10.03.2025 (Online Registration & Online Payment) Date of Examination Will be intimated later 3. SCALE OF PAY: Pay matrix Level-11 - Rs.35,400 – 1,30,400

MCQ discussion in Online Class for - DRUGS INSPECTOR EXAMS - RRB PHARMACIST EXAM - CRE AIIMS PHARMACIST - GPAT - DPEE - D.PHARM - B.PHARM - PHARM. D.
Introduction Pharmacy is a rapidly growing field in India, offering numerous opportunities for students who aspire to build a career in healthcare, research, and the pharmaceutical industry. Competitive exams in pharmacy serve as a gateway to higher education, government jobs, and lucrative careers in multinational companies. Some of the most sought-after pharmacy entrance and competitive exams and recruitment exams in India include the Graduate Pharmacy Aptitude Test (GPAT), NIPER Joint Entrance Exam (NIPER JEE), Entrance Exams for many Deemed and Private Universities, Common University Entrance Test - CUET (UG), Drug Inspector Exams, Drug Controller Exams, Exams for Academic and Research Posts in Universities and Colleges, Pharmacist Recruitment Exams, etc. conducted by Union Public Service Commission, State Public Service Commissions and various boards such as Railway Recruitment Board (RRB). Preparing for these competitive exams requires a well-structured plan, dedication, and effective study strategies. In this blog, we will explore essential tips and strategies to help pharmacy aspirants excel in these exams. Understanding the Exam Pattern and Syllabus Before diving into preparation, it is crucial to understand the exam pattern and syllabus of the specific exam you are targeting. Here is a brief overview of some major pharmacy competitive exams: 1. GPAT (Graduate Pharmacy Aptitude Test) • Conducted by the National Testing Agency (NTA), GPAT is the gateway to M. Pharmacy programs in India. • It consists of 125 multiple-choice questions (MCQs) with a total of 500 marks. • The syllabus includes subjects like Pharmaceutics, Pharmaceutical Chemistry, Pharmacology, and Pharmacognosy. • Negative marking is applicable. 2. NIPER JEE (National Institute of Pharmaceutical Education and Research Joint Entrance Exam) • Conducted by NIPER for admission into M. Pharm, PhD, and MBA (Pharm.) programs. • The syllabus covers GPAT topics along with additional topics like Biopharmaceutics, Biotechnology, and Pharmacokinetics. • The exam is highly competitive and requires in-depth conceptual understanding. 3. Drug Inspector & Pharmacist Recruitment Exams • Drug Inspector Exams are conducted by UPSC at central level and State Public Service Commissions (PSC) at state levels. • Pharmacist Recruitment Exams for Government sectors are conducted by various government bodies and boards such as CRE-AIIMS and RRB. • The syllabus includes Pharmacy Act, Drugs and Cosmetics Act, Pharmacology, Pharmaceutics, topics from B.Pharmacy syllabus as professional subject and non professional subject may include General Knowledge, Intelligence Quotient (I.Q.), aptitude and reasoning, Mathematics, English and Official language of the state. Exam pattern and syllabus may vary and depend on Exam Conducting Authorities. but usually includes objective-type questions. Normally, these exams are MCQ based Computer Based Test (CBT). • Sometimes, Personal Interviews may be conducted after qualifying the CBT. • For army and related organizations, Physical Fitness Test is a compulsion. Effective Preparation Strategies 1. Create a Study Plan • Set a realistic timetable and stick to it. • Allocate time for each subject based on its weightage in the exam. • Include revision slots in your schedule. 2. Refer to Standard Books • Use books recommended by experts for conceptual clarity: o Pharmaceutics - Remington: The Science and Practice of Pharmacy o Pharmaceutical Chemistry - Morrison and Boyd (Organic Chemistry) o Pharmacology - Rang & Dales Pharmacology o Pharmacognosy - Trease and Evans Pharmacognosy • NCERT Biology books (Class 11 & 12) can be helpful for basic understanding. 3. Use Online Resources and Coaching Materials • Many online platforms offer mock tests, video lectures, and practice papers. • Websites like www.pharmalifeacademy.com provides valuable study materials in the form of blogs by the experts on a particular topic and test packages to boost your preparation. • Preparing own notes and self study is the MANTRA for the success in any exam. Taking support from teachers, faculties and coaching institutes such as Pharmalife Academy will prepare you better. 4. Practice Mock Tests and Previous Year Papers • Solving previous years question papers helps in understanding the exam pattern and identifying important topics. • Take timed mock tests regularly to improve speed and accuracy. You can find such tests on www.pharmalifeacademy.com • Analyze mistakes and work on weak areas. 5. Revise Regularly • Make short notes for quick revision. • Revise formulas, structures, and classification tables frequently. • Use flashcards for memorizing key points. 6. Stay Updated with Current Affairs and General Knowledge • For exams like Drug Inspector and Pharmacist recruitment, general knowledge and current affairs play a crucial role. • Read newspapers, follow government notifications, and stay updated with new developments in the pharmaceutical industry. Maintaining Motivation and Managing Stress Competitive exams require months of dedicated preparation, which can sometimes be overwhelming. Here are some tips to stay motivated and manage stress: 1. Set Realistic Goals • Break your preparation into smaller milestones. • Reward yourself after achieving each goal. 2. Follow a Healthy Routine • Ensure adequate sleep and a healthy diet. • Engage in physical activities like yoga or meditation to reduce stress. • Avoid excessive screen time and social media distractions. 3. Join Study Groups and Discuss with Peers • Group discussions help in better understanding of complex topics. • Explaining concepts to others reinforces your own learning. • Join online forums or Telegram groups related to pharmacy exams. 4. Stay Positive and Confident • Believe in yourself and your preparation. • Do not compare your progress with others; focus on self-improvement. • Develop a positive mindset to overcome challenges. Conclusion Preparing for competitive pharmacy exams in India requires a strategic approach, disciplined study routine, and strong conceptual knowledge. Understanding the syllabus, using the right study materials, practicing mock tests, and staying motivated are key elements of success. With consistent effort and the right mindset, you can achieve your goals and secure a bright future in the field of pharmacy. Stay focused, stay positive, and give your best in the exam!
MCQ discussion in Online Class for - RRB PHARMACIST EXAM - CRE AIIMS PHARMACIST - GPAT - DRUGS INSPECTOR EXAMS - DPEE - D.PHARM - B.PHARM - PHARM. D. To watch the discussion
* After studying this topic, attempt a test on METFORMIN under the category ‘TEST FOR YOU: TOPIC-WISE on the TEST PACKAGES page. This blog prepares you for GPAT D.Pharm, B.Pharm, and Pharm.D. (Pharmacy Exams) RRB Pharmacist Recruitment Exam Common Recruitment Examination for AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE Medical and Nursing Exams Metformin is recommended as the first line treatment in type 2 diabetes in adult and pediatric patients 10 years and older. Metformin belongs to biguanide class of oral hypoglycaemic agent. Metformin decreases hepatic gluconeogenesis production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization. It does not stimulate insulin secretion. As monotherapy, it rarely produces hypoglycaemia. The recommended starting daily dose is 500 mg after meals, which is increased by 500 mg every two weeks until desired therapeutic goals are achieved or maximum daily doses (2500 mg) are reached. The usual daily dosage range for Metformin SR is 500 mg to 2000 mg, taken once or twice a day. It can be used in combination with any other oral or injectable anti-hyperglycaemic agents. Metformin is quickly absorbed from the small intestine. Bioavailability is from 50% to 60%, and the drug is not protein bound. Metformin is excreted as unmetabolized drug in the urine, via tubular excretion. It is advisable to stop metformin at least 24 hours before major surgery or use of radio contrast media. Its adverse reaction includes lactic acidosis, megaloblastic anemia, diarrhea, myalgia, abdominal pain, Vitamin B12 deficiency, etc. Monitoring of blood glucose levels as an effect of metformin can be easily done hence therapeutic drug monitoring is not required for metformin. Metformin is contraindicated in patients with metabolic acidosis. Generally avoid metformin use in hepatic impairment; hepatic disease increases the risk of metformin-associated lactic acidosis. Symptoms of overdosage include lactic acidosis manifested as malaise, myalgia, respiratory distress, increasing somnolence and abdominal distress. Drug interactions include I) Increased risk of lactic acidosis with carbonic anhydrase inhibitors, NSAIDs, ACE inhibitors, angiotensin II receptor antagonists and loop diuretics. II) Competitive inhibition of renal excretion of metformin by cimetidine, which can lead to increased metformin blood levels. Phenformin and buformin are derivatives of metformin. These two drugs were withdrawn from the market due to toxic lactic acidosis effects and an increased incidence of cardiac mortality. Metformin is often a second-line treatment for menstrual irregularity in PCOS patients, particularly those who are unable to take or tolerate combined oral contraceptives, or those who have insulin resistance. It is a white crystalline powder, almost odourless, freely soluble in water and less in alcohol. It is hygroscopic in nature. Storage: It is hygroscopic in nature and so it is stored in a tightly closed container. Some popular brand names of metformin are Metformin, Glycomet, Glyciphage, Diabex, Diaformin, DMGG. MCQs 1. Which of the following antidiabetic drug (oral) does not stimulate insulin secretion? a) Metformin b) Nateglinide c) Repaglinide d) Glyburide 2. Which of the following are common side effects of Metformin? a) Diarrhea, mild gastrointestinal distress, and lactic acidosis b) Nausea, severe abdominal pain, and hypertension c) Dizziness, skin rash, and liver failure d) Weight gain, dizziness, and hyperglycemia To proceed with the TEST ON METFORMIN,
उत्तराखंड अधीनस्थ सेवा चयन आयोग ने फार्मासिस्ट (कारागार विभाग) के पदों पर भर्ती के लिए अधिसूचना जारी की The Uttarakhand Subordinate Service Selection Commission has released a notification for the recruitment of Pharmacist (Prison Department) positions. The Uttarakhand Subordinate Service Selection Commission (UKSSSC) has issued a recruitment notification (Advertisement No. 68/UKSSSC/2025) for Pharmacist (Prison Department) positions. The application process began on February 6, 2025, and will close on February 28, 2025. उत्तराखंड अधीनस्थ सेवा चयन आयोग (UKSSSC) ने फार्मासिस्ट (कारागार विभाग) के पदों पर भर्ती के लिए अधिसूचना (विज्ञापन संख्या 68/UKSSSC/2025) जारी की है। आवेदन प्रक्रिया 6 फरवरी 2025 से शुरू हो चुकी है और 28 फरवरी 2025 को समाप्त होगी। To download the advertisement and syllabus:
The ECHS has announced vacancies for contractual appointments of pharmacist at its polyclinics across multiple regional centers across India. The dates for application submissions and interviews vary by location. Salary: 28,100/- per month Link to Download Application Form and Terms and Conditions:
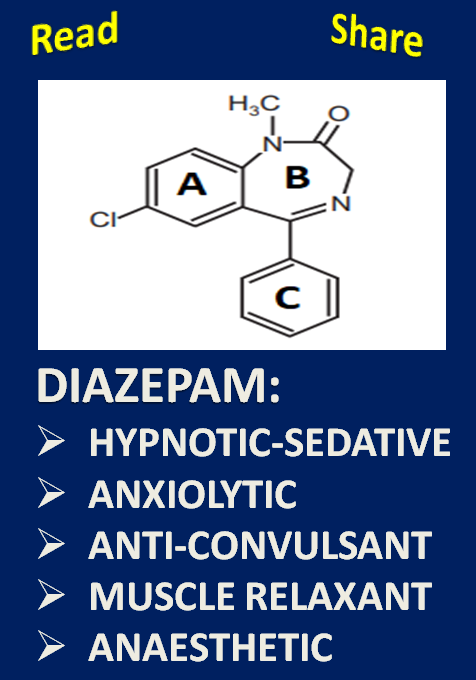
* After studying this topic, attempt a test on DIAZEPAM under the category ‘TEST FOR YOU: TOPIC-WISE on the TEST PACKAGES page. This blog prepares you for GPAT D.Pharm, B.Pharm, and Pharm.D. (Pharmacy Exams) RRB Pharmacist Recruitment Exam Common Recruitment Examination for AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE
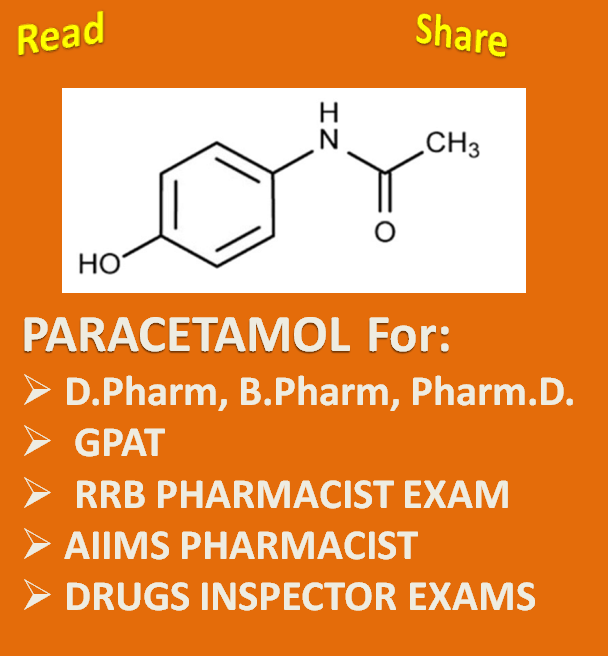
* After studying this topic, attempt a free test on PARACETAMOL under the category ‘TEST FOR YOU: TOPIC-WISE on the TEST PACKAGES page. PARACETAMOL for GPAT D.Pharm, B.Pharm, and Pharm.D. (Pharmacy Exams) RRB Pharmacist Recruitment Exam Common Recruitment Examination for AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE

This online class prepares you for > GPAT > RRB PHARMACIST EXAM > CRE AIIMS PHARMACIST > DRUGS INSPECTOR EXAMS > DPEE > D.PHARM > B.PHARM > PHARM. D. To watch the class
The CRE AIIMS Pharmacist exam is one of the most competitive exams for those aspiring to build a career as a pharmacist at one of the most prestigious government health institutions. As the exam date approaches, it is natural to feel a mix of anticipation and anxiety. But do not worry! The final days of preparation can still make a significant difference if you use them strategically. Here are some effective tips to help you make the most of your remaining days of preparation:

* After studying this topic, attempt a test on ASPIRIN under the category ‘TEST FOR YOU: TOPIC-WISE on the TEST PACKAGES page. Aspirin for GPAT D.Pharm, B.Pharm, and Pharm.D. (Pharmacy Exams) RRB Pharmacist Recruitment Exam Common Recruitment Examination for AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE • Aspirin is a NON STEROIDAL ANTI-INFLAMMATORY (NSAID) agent. • Aspirin has analgesic, antipyretic, anti-inflammatory and antiplatelet effects. • It belongs to the SALICYLATE class of NSAID drugs. • Chemically, it is ACETYLSALICYLIC ACID and 2-ACETOXYBENZOIC ACID is its IUPAC name. • The name Aspirin was given to Acetylsalicylic acid by BAYER, a German Pharmaceutical Company. • Aspirin is an International Non-proprietary (INN) name or Generic name. • Aspirin is hygroscopic, white crystal or crystalline powder, odourless with slightly bitter taste and is water soluble. • Esterification reaction is involved in the synthesis of aspirin. • Aspirin is a weakly acidic drug and remains unionised in an acidic environment. So, it is lipid soluble when the medium has low pH. • The carboxyl group of aspirin after esterification with N-acetyl p-amino phenol gives 4-acetamidophenyl-O-acetyl salicylate. • Acetylsalicylic acid is rapidly converted in the body to salicylic acid. • Aspirin is a NON-SELECTIVE COX (cyclooxygenase) inhibitor. • It is THROMBOXANE SYNTHESIS INHIBITOR type of ANTIPLATELET AGENT. • Platelets produce Thromboxane A2 that enhances platelet aggregation. • Aspirin inhibits platelet aggregation by irreversibly inhibiting COX-1 in platelets which results in inhibition of all of the thromboxane production by platelets. Thus, it increases the bleeding time. • NSAID except aspirin does not affect platelet aggregation because aspirin inhibits COX irreversibly while other NSAIDs are reversible COX inhibitors. Also, aspirin has more potency against COX-1 enzyme. • Depending on the dose, adverse effects of aspirin on G.I. tract may be INDIGESTION, HEARTBURN, STOMACH PAIN, NAUSEA AND VOMITING, DIARRHOEA OR CONSTIPATION, STOMACH IRRITATION AND ULCERS, AND GASTROINTESTINAL (GI) BLEEDING. Aspirin is contraindicated in peptic ulcer. • In airways, arachidonic acid gets converted to prostanoids by COX enzymes and leukotrienes by 5‐lipoxygenase (LOX) enzymes. Prostanoids are bronchodilators while leukotrienes are bronchoconstrictors. Aspirin can block the production of prostanoid but not of the leukotrienes. Thus, there will be no bronchodilation; only bronchospasm will be there. This is especially true for asthmatics. This is why aspirin is a trigger factor for asthma and is contraindicated in asthma. • Aspirin may cause REYES SYNDROME in children <16 years recovering from viral infection. • AT HIGH DOSES (3-5 gm/day or 100 mg/kg/day) needed for anti-inflammatory action in rheumatoid arthritis/rheumatic fever aspirin produces the following effects: 1) Respiration: Respiration is stimulated as a result of i) Increase consumption of oxygen primarily by the skeletal muscles leading to increased production of carbon dioxide which directly stimulates the respiratory centre. ii) Direct stimulation of the medullary respiratory centre. iii) Chemoreceptors stimulation. 2) Hepatic and renal effects: Aspirin can affect renal function in damaged kidneys by inhibiting COX-1. Large doses of aspirin particularly in children can cause hepatic damage and even necrosis. 3) Uricosuric effect: In small doses (1-2 g per day), aspirin interferes with urate excretion, increases the plasma urate level, and blocks the action of other uricosuric drugs such as probenecid. In large doses (≥ 5 gm/day) it may block urate reabsorption by nephron. This results in uricosuria. 4) Metabolic effects: Toxic doses of aspirin may lead to hyperpyrexia, increased protein catabolism, aminoaciduria and a negative nitrogen balance. Glucose utilization is increased resulting in hypoglycemia especially in diabetics. Toxic doses may cause central sympathetic stimulation and hyperglycemia. • Aspirin may produce METHEMOGLOBINEMIA and TINNITUS. • ASPIRIN: INDICATIONS AND DOSAGE Aspirin: As analgesic-antipyretics: Oral: 300-900 mg, repeated 4-6 hourly according to clinical needs. Prophylaxis of cardiovascular events in high-risk patients: Oral: 75-150 mg once daily. • SALICYLISM: Antiinflammatory doses (3–5 gm/day) of aspirin may produce a condition of mild salicylate intoxication termed salicylism. It is characterized by headache, dizziness, vertigo, tinnitus, reversible impairment of hearing and vision, drowsiness, lethargy and mental confusion, excitement, nausea, vomiting, diarrhoea hyperventilation and electrolyte imbalance. These symptoms may be associated with tachypnoea and respiratory alkalosis. It is reversible on stoppage of therapy. • ACUTE SALICYLATE POISONING: Acute salicylate poisoning may be due to accidental ingestion in children. In adults, fatal dose is estimated to be 15-30 gm. Symptoms of acute intoxication are vomiting, dehydration, acid-base and electrolyte disturbances, hyperpyrexia, hyper/hypoglycaemia, GI irritation and occasional haemorrhages, restlessness, delirium, vertigo, tremor, apprehension, hallucinations, convulsions, coma and death due to respiratory failure and cardiovascular collapse. • Salicylate therapy is always supported with vitamin K. • SODIUM BICARBONATE is the antidote for salicylate poisoning. CONTRAINDICATIONS FOR ASPIRIN INCLUDE • Hypersensitivity • Peptic ulcer, • Haemorrhagic disease, coagulation disorder (e.g. haemophilia, thrombocytopenia) • Gout • Severe hepatic and renal impairment • Children <16 years and recovering from viral infection. • Pregnancy (doses >100 mg daily during 3rd trimester) and lactation. • Concomitant use with other NSAIDs and methotrexate. • Aspirin + Paracetamol as analgesic – antipyretic is an ADDITIVE combination. • Codeine and aspirin as analgesics is a SYNERGISTIC combination. • Aspirin blocks the uricosuric action of probenecid and decreases tubular secretion of methotrexate. • Storage condition: It is hygroscopic so it should be stored in air tight containers, in a cool, dry place. • Ecosprin, Disprin, Equagesic, Acetosal, Acetylin, Aspro, Saletin, Caprin, Asteric are some of its popular brand names. MCQs 1. Aspirin poisoning includes following symptoms EXCEPT: a) Dehydration b) Hypothermia c) Metabolic acidosis d) Oliguria 2. Among all NSAIDs, only aspirin has a significant antiplatelet effect because _______. a) Aspirin inhibits COX 1 irreversibly. b) Aspirin inhibits COX 1 reversibly. c) Aspirin blocks COX 1 less than COX 2. d) Aspirin is a salycilate. To proceed with the TEST ON ASPIRIN,

Traditionally, the pharmacy profession has been associated with the development, manufacturing, and distribution of high-quality drug products with guaranteed effects. However, with the introduction of new courses, curricula, training, and the evolving needs of the time, the scope and responsibilities of the pharmacy profession have expanded significantly. Today, pharmacists are recognized as experts in medicines. Considering the growth of the healthcare sector in India, pharmacists with qualifications such as D.Pharm, B.Pharm, M.Pharm, Pharm.D., or Ph.D. have numerous career opportunities. Additionally, exams like GPAT (Graduate Pharmacy Aptitude Test) and Diploma in Pharmacy Exit Exam (DPEE) open doors to various government and private sector roles. However, to take full advantage of these opportunities, pharmacist must adapt to the ever-increasing demand for effective communication, in-depth knowledge, innovation, research skills, and overall expertise required in the profession. This blog will highlight some of the common career options in pharmacy profession. 1. Community Pharmacist One of the most common career paths for registered pharmacists is working as a community pharmacist. With a D.Pharm or B.Pharm degree, you can work at retail pharmacies, or set up your own pharmacy business. Entrepreneurship opportunities are also growing in the community pharmacy sector, especially with the rise of online pharmacies and telemedicine. 2. Hospital Pharmacist Hospital pharmacists are an integral part of the healthcare team. In India, there are currently hundreds of vacancies for hospital pharmacists in the government sector. Various government hospitals, institutions, organizations, and bodies—such as the Railway Recruitment Board (RRB), All All India Institute of Medical Sciences (AIIMS), Indian Air Force, Directorate of Health Services (DHS), Directorate of Medical Education and Research (DMER), Zilla Parishads, Municipal Corporations, ISRO, RBI, SBI, and public sector companies—conduct Pharmacist Recruitment Exams to fill these positions. Typically, a registered pharmacist with a D.Pharm, B.Pharm, or Pharm.D. qualification is eligible to apply for these government jobs in India. 3. Clinical Pharmacist Clinical pharmacists work directly with healthcare teams in hospitals or clinical settings to provide expert advice on the safe and effective use of medications. Clinical pharmacists play a crucial role in improving patient outcomes by managing drug regimens and preventing adverse drug reactions. In India, this career path typically requires a Pharm.D. along with clinical experience. 4. Marketing Jobs as Medical Representative Marketing jobs as Medical Representatives (MR) offer an exciting opportunity for pharmacy graduates. As a Medical Representative, you will be responsible for promoting pharmaceutical products to healthcare professionals, hospitals, and clinics. This career path offers competitive salaries, travel opportunities, and the chance to work with major pharmaceutical companies, making it an appealing option for many pharmacy graduates. 5. Industrial Pharmacist The pharmaceutical industry offers various roles for pharmacy graduates, including positions in drug manufacturing, quality control, production, and formulation development. As an industrial pharmacist, you can work with pharmaceutical companies to develop new drugs, ensure compliance with regulatory standards, or manage production lines. A B.Pharm or M.Pharm, coupled with industry-specific knowledge, opens doors to exciting opportunities. 6. Regulatory Jobs Regulatory affairs is an essential part of the pharmaceutical industry. Regulatory affairs professionals ensure that drugs, medical devices, and related products meet all the required legal and safety standards. Indian regulatory bodies like the CDSCO (Central Drugs Standard Control Organization) and FDA play a crucial role in approving medicines and ensuring their safety. The path to regulatory jobs may involve passing exams such as the Drugs Inspector Exams. A fresher pharmacy graduate is eligible to apply for the post of Drugs Inspector. There are many other attractive job opportunities for pharmacy graduates, such as in pharmacovigilance, medical coding, clinical research, pharmacy-related legal services, pharmacy journalism, and more.
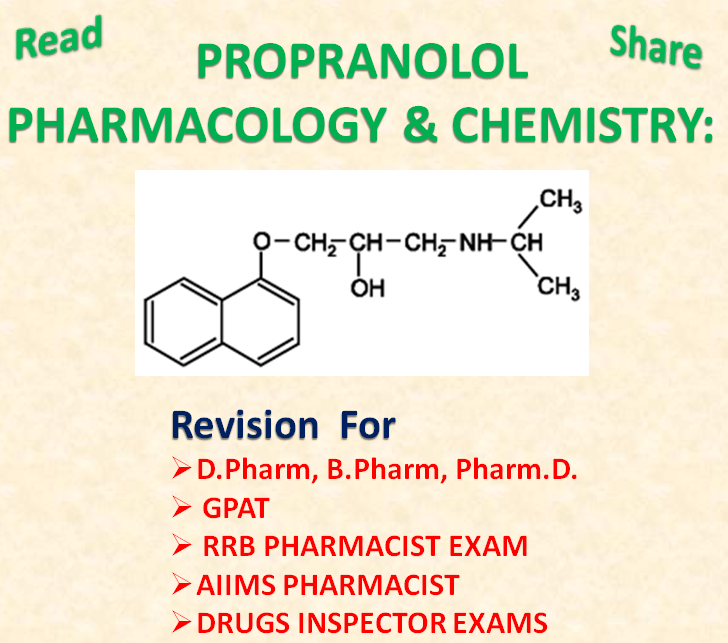
* Do not miss the test on this topic on the TEST PACKAGES page. Revision for GPAT RRB Pharmacist Recruitment Exam Common Recruitment Examination for AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE D.Pharm, B.Pharm, and Pharm.D. Exams • Propranolol is a non-selective β adrenergic blocker without intrinsic sympathomimetic activity. • It is a competitive antagonist at β adrenergic receptors. • It blocks ß1 and ß2 receptors but has weak activity on ß3 subtype. • It is also an inverse agonist. It reduces resting heart rate as well. • Propranolol is a white crystalline powder, almost odourless and bitter in taste. Pharmacological Actions of Propranolol (Prototype of β-Blockers): (i) Propranolol decreases heart rate, force of contraction and cardiac output (c.o.). (ii) It has direct depressant effect on heart due to membrane stabilizing action at higher doses. (iii) In angina patients, it improves oxygen supply / demand status. (iv) It decreases renin release from kidney ( β1 mediated) causing a fall in BP. (v) On prolonged administration of propranolol BP gradually falls in hypertensive subjects but not in normotensive. (vi) It can cross the blood brain barrier. It produces minute behavioural changes, forgetfulness, increased dreaming and nightmares with long-term use of relatively high doses. It suppresses anxiety in short term stressful situations. (vii) Propranolol is a potent local anaesthetic, but is not clinically used for this purpose because of its irritant property. (viii) Prolonged propranolol therapy may reduce carbohydrate tolerance by decreasing insulin release. (ix) Plasma triglyceride level and LDL/HDL ratio is increased during propranolol therapy. (x) Instillation of propranolol reduces secretion of aqueous humor, intraocular tension is lowered. Pharmacokinetics: Propranolol is well absorbed after oral administration but has low bioavailability due to first pass metabolism in liver. It is lipophilic and penetrates into brain easily. • Propranolol is indicated for hypertension; angina pectoris; cardiac arrhythmias; myocardial infarction; CHF; glaucoma. • It is a Class II antiarrhythmic drug. • It is used as prophylaxis of migraine, thyrotoxicosis, anxiety. • Propranolol is contraindicated in bronchial asthma, COPD, bradycardia, hypotension, Prinzmetal angina. • Propranolol brand names: Inderal, InnoPran XL. MCQs 1. All of the following statements related to propranolol are correct, except _____. a) It cannot cross blood brain barrier. b) In angina patients, it improves oxygen supply/demand status. c) Propranolol suppresses anxiety in short term stressful situations. d) Propranolol is as potent a local anaesthetic as lidocaine. 2. Select the drug contraindicated in Asthma. a) Quinidine b) Propranolol c) Salbutamol d) Paracetamol To proceed with the TEST ON PROPRANOLOL
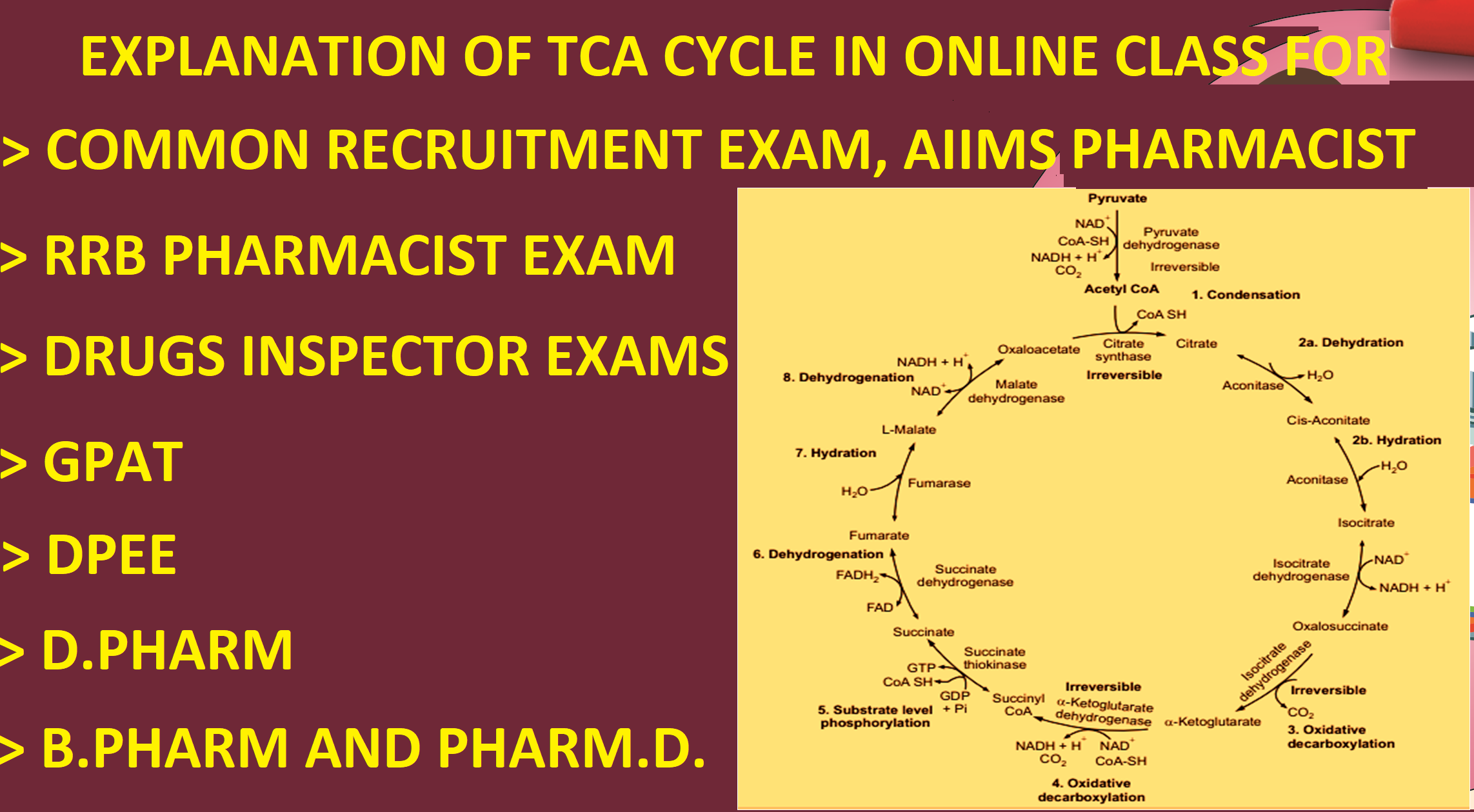
This online class prepares you for > GPAT > RRB PHARMACIST EXAM > COMMON RECRUITMENT EXAM, AIIMS PHARMACIST > DRUGS INSPECTOR EXAMS > DPEE > D.PHARM > B.PHARM > PHARM. D. To watch the class
* Do not miss the test on this topic on the TEST PACKAGES page. This blog prepares you for GPAT D.Pharm, B.Pharm, and Pharm.D. Exams RRB Pharmacist Recruitment Exam Common Recruitment Examination for AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE Adrenergic receptors (α and β receptors) are the receptors which mediate the actions of noradrenaline (norepinephrine) and adrenaline (epinephrine). All of the adrenergic receptors are membrane bound G-protein coupled receptors. Adrenergic receptors function primarily by increasing or decreasing the intracellular production of second messengers cAMP or IP3/DAG. In some cases the activated G-protein itself operates K+ or Ca2+ channels, or increases prostaglandin production. The adrenergic receptors are classified on the basis of their apparent drug sensitivity. They are classified as α and β-receptors. α-receptors are further subdivided as α1 and α2. α1A, α1B, and α1D are subtypes of α1 receptors. α2A, α2B, and α2C are subtypes of α2 receptors. β-receptors are subdivided as β1, β 2, and β 3 receptors. The rank order of agonist potency for α-receptors is epinephrine > norepinephrine >> isoproterenol. The rank order of agonist potency for β -receptors is isoproterenol > epinephrine > norepinephrine. The α1 receptor is a G-protein coupled receptor generally an excitatory receptor connected to the Gq G-protein. The α1 receptors can be thought of as a receptor of contraction. α1 receptors are found at: vascular smooth muscles, bronchial smooth muscle, radial smooth muscles of iris, pilomotor smooth muscles, prostate, urinary bladder and anal sphincter, mucous membrane, uterus and in the CNS neurons. The α2 receptor is an inhibitory G-protien coupled receptor connected to the Gi G-protein. Once activated by the α2 receptor, Gi inhibits adenylyl cyclase, and cause intracellular cAMP levels to decrease. Within sympathetic nervous system, α2 receptors are found on the presynaptic terminals of postganglionic sympathetic neurons and inhibit further release of norepinephrine. α2 receptors are the primary adrenergic receptor within the CNS. α2 receptors are also found at pancreatic islets which cause inhibition of insulin release and at platelets cause platelet aggregation. All of the β receptors are generally excitatory GPCR connected to the Gs G-protein. Stimulation of β receptor activates Gs G-protein which then activates adenylyl cyclise and the generation of intracellular cAMP. This starts a chain of events that lead to the effects of β receptor activation. β1 receptors are typically found at myocardium in the heart and juxtaglomerular cells in kidneys. They are also found in the CNS and adipose tissues. The most important effects of stimulation of beta1 receptors are: o Increased heart rate and contractility. o Increased release of renin. o In the CNS, it causes ADH secretion from posterior pituitary gland that enhances renal salt and water reabsorption. o In adipocytes, it enhances lipolysis. β2 receptors are typically found at bronchi, blood vessels, uterus, liver, G.I.T., urinary tract, eye. They are not predominant in the heart. The physiological action of β2 receptors is mainly due to relaxation of smooth muscle and modulation of hepatic metabolism. Their activation causes bronchodilation, vasodilation, low B.P., uterine relaxation, stimulation of glycogenolysis and gluconeogenesis, increased blood glucose concentration. β3 receptors are typically found at adipose tissue and detrusor muscle of bladder. Their activation increase lipolysis and urinary bladder relaxation. MCQs 1. The receptors which mediate the action of epinephrine or norepinephrine are ____ a) Adrenergic receptors b) Nephrogenic receptors c) Cholinergic receptors d) Angiotensin receptors 2. All of the adrenergic receptors are ______ a) G-protein coupled receptors b) Ion channel receptors c) Enzyme linked receptors d) Nuclear receptors To proceed with the TEST ON ADRENERGIC RECEPTORS,
* Do not miss the test on this topic on the TEST PACKAGES page. This blog prepares you for GPAT D.Pharm, B.Pharm, and Pharm.D. Exams RRB Pharmacist Recruitment Exam Common Recruitment Examination for AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE • Adrenaline and noradrenaline are also known as epinephrine and norepinephrine respectively. • Adrenaline and noradrenaline are hormones and neurotransmitters produced by the adrenal glands and adrenergic nerve endings. • As a neurotransmitter, adrenaline and noradrenaline are involved in sympathetic nervous system. • Adrenaline and noradrenaline are direct acting sympathomimetic agents. They bind to and activate adrenergic receptors directly. • Adrenaline has α1, α2, β1, β2 and weak β3 action. • Noradrenaline has α1, α2, β1, β3 but no β2 action. • Tyrosine is considered to be the precursor for the biosynthesis of noradrenaline. • The enzyme involved in the conversion of noradrenaline to adrenaline is N-methyltransferase. • Adrenaline and noradrenaline are catecholamines. • The structural difference between adrenaline and noradrenaline is the presence of an N-methyl group in adrenaline, which is absent in noradrenaline. (See structures) • Noradrenaline is a white or brownish white crystalline powder, soluble in water. • Adrenaline is a white microcrystalline powder, soluble in water. Pharmacological Actions of Adrenaline • Heart: Adrenaline with its action on β1-receptors of heart increases heart rate (positive chronotropic), force of contraction (positive inotropic), conduction velocity (positive dromotropic) and cardiac output. It may produce ventricular arrhythmia. • Blood Vessels: Both vasoconstriction (through α1 receptor) and vasodilatation (through β2 receptor) can occur depending on the dose and the vascular bed. Vasoconstriction occurs peripherally in skin, mucous membrane and renal beds. Vasodilatation predominates in skeletal muscles, liver and coronaries. • Blood Pressure: Adrenaline by slow IV infusion or SC injection causes rise in systolic BP (by myocardial action) but fall in diastolic BP. The reason for this fall in diastolic BP is more sensitivity of vascular β2 receptors than α1 receptors. In animals, rapid IV injection of adrenaline produces biphasic response. Initially, it causes peripheral vasoconstriction and leads to rise in systolic BP. This is followed by dilation of skeletal muscle blood vessels, decrease in resistance and output, and fall in diastolic BP. This response of adrenaline is known as biphasic response. Dales vasomotor reversal: If vasoconstriction action of adrenaline is blocked by α1 blocker, it causes only fall in BP. This reversal of action of adrenaline from biphasic to monophasic response on blood pressure is called as Dales vasomotor reversal. • Smooth Muscles: Adrenaline relaxes smooth muscles due to action on β2 receptors. It is a powerful bronchodilator. • Central Nervous System: In clinically used doses adrenaline may produce tremors, restlessness, palpitation and apprehension. • Eye: Topical application of adrenaline may cause mydriasis and fall in intraocular tension. • Metabolism: (i) Adrenaline causes glycogenolysis leading to hyperglycaemia and hyperlactacidaemia. (ii) It also causes lipolysis which leads to increase in plasma free fatty acid (FFA) and calorigenesis (β2 + β3). (iii) In addition metabolic effects result from reduction of insulin and augmentation of glucagon secretion. • Antiallergic Actions: Adrenaline is a physiological antagonist of histamine and counters the bronchoconstriction and hypotension of anaphylactic shock. • Adrenaline is orally inactive because it is rapidly degraded by monoamine oxidase (MAO) and catechol O methyl transferase (COMT) present in the intestinal wall and liver. • MAO causes the intraneuronal metabolism of catecholamines and COMT causes extraneuronal metabolism of catecholamines. • Adrenaline can treat a number of life threatening medical emergencies such as anaphylactic shock, asthma and bronchospasm, cardiac shock, severe upper airway obstruction, uncontrolled bleeding, etc. • Its peripheral vasoconstrictor property can be used to stop nasal and dental bleeding. • Adrenaline is given along with local anaesthetics to produce local anaesthesia because adrenaline causes peripheral vasoconstriction resulting in (i) decreased systemic absorption of local anesthetics, (ii) prolonged duration of action of local anesthetics, (iii) decreased dose of local anaesthetics and (iv) decreased systemic toxicity of local anaesthetics. • Adrenaline with local anaesthetics is a synergistic combination. • Noradrenaline (Norepinephrine, levarterenol): Noradrenaline causes rise in systolic, diastolic and mean BP. It increases peripheral resistance consistently due to α action. It doesn’t have β2 action (vasodilation). It is a drug of choice for acute hypotensive shock. • Hypertension, hyperthyroid, angina patients, occlusive vascular disease, hypersensitivity, cardiac arrhythmias or tachycardia, angle-closure glaucoma (eye drops) are some of the contraindications for adrenaline. SAR of Phenylethanolamine Adrenergic Agonists (See structures) Adrenaline and noradrenaline are phenylethanolamine. In phenylethanolamine adrenergic agonists, a primary or secondary aliphatic amine separated by two carbons from a substituted benzene ring is minimally required for high agonist activity. These agents also have a hydroxyl group on C1 of the side chain, β to the amine, as in adrenaline and noradrenaline. Stability and Storage Conditions of Adrenaline • Adrenaline can be oxidized by air or oxygen to get pink or red colour complex. • It darkens on exposure to light and air. • It is stored in tightly closed light resistant containers. MCQs 1. Identify the incorrect statement: Adrenaline is added to local anaesthetics to _____. a) enhance bioavailability of local anaesthetics b) prolong the duration of action of local anaesthetics c) reduce the systemic absorption of local anaesthetics d) reduce systemic toxicity of local anaesthetics 2. Secondary amine is a part of___ a) Adrenaline b) Noradrenaline c) Dopamine To proceed with the TEST ON ADRENALINE & NORADRENALINE,

* Do not miss the test on this topic on the TEST PACKAGES page. This blog prepares you for GPAT RRB Pharmacist Recruitment Exam Common Recruitment Examination for AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE D.Pharm, B.Pharm, and Pharm.D. Exams • Atropine is a prototype anticholinergic/antimuscarinic/parasympatholytic drug. • It blocks the action of acetylcholine by blocking the muscarinic cholinergic receptors. • It does not block nicotinic cholinergic receptors. • It is a naturally occurring tropane alkaloid that is found in Atropa belladonna and Hyocyamus niger. • Atropine is a racemic mixture of l-hyoscyamine and d-hyoscyamine. • It occurs as colourless crystals or white crystalline powder. It is odourless and has bitter taste. • Atropine is official as sulphated salt which contains one molecule of water of crystallization. • Atropine has low solubility in water but its official salt, atropine sulphate is very soluble in water. • It is an amino alcohol ester. It is composed of a tropine (an amino alcohol) and a tropic acid (a carboxylic acid), which form an ester bond (see image). • In acidic or alkaline medium, it is hydrolyzed to give tropine and tropic acid. • Storage condition: It is required to be kept in well closed containers, protected from light. Pharmacological Actions of Atropine • Pharmacological actions of atropine are observed mainly because it competitively antagonizes acetylcholine at the muscarinic receptor. • Atropine doesn’t affect the nicotinic actions of acetylcholine at autonomic ganglia and skeletal muscles. • Effect on secretions: Atropine reduces the volume and total acidity of gastric secretions. It also reduces salivary secretion (salivary glands secretion), secretions in nose, pharynx, and bronchi. It also reduces the sweat secretion. • Effect on smooth muscles: Usually, atropine relaxes all smooth muscles such as that of gastrointestinal tract, urinary tract, bronchi, etc. • Atropine stops excessive tone and motility of gastrointestinal tract. It does not interfere with normal peristalsis. • Atropine reduces normal as well as drug induced ureteral peristalsis. It reduces tone of bladder muscles and tends to produce urinary retention. • Atropine is effective in relieving the bronchospasm produced by cholinergic drugs. • Effect on eye: On local instillation, atropine produces mydriasis by blocking the cholinergic nerve supply. It causes photophobia and ‘Paralysis of accommodation’ that is known as ‘Cycloplegia’. • Effect on cardiovascular system: Atropine in therapeutic doses may initially decrease the heart rate because it has partial agonist property with acetylcholine. But it is followed by tachycardia. Toxic doses of atropine produce cutaneous vasodilation resulting in atropine flush and hypotension. • Effect on CNS: Atropine in therapeutic doses stimulates the medullary vagal nuclei. This causes increase in rate and depth of respiration. At low doses, it causes slight restlessness; and at high or toxic doses it causes restlessness, agitation, hallucination. Important Dosage, Indications and Contraindications of Atropine • Bradycardia: 1 mg every 3 to 5 minutes upto a max. total dose of 3 mg I.V. (Adult). Repeat the doses until obtaining the desired effects. • As preanaesthetic agent: 2 mg oral/0.2 to 1 mg I.V., I.M., or S.C. 30 to 60 min prior to anesthesia. • Antisialogogue/Antivagal: 0.5 mg to 1 mg every 1 to 2 hours I.V. (Adult) • Organophosphate/Muscarinic poisoning: 2 to 3 mg every 20 to 30 min I.V. (Adult) • Irritable bowel syndrome, non-ulcer dyspepsia and diverticular disease: Adult: 0.6 to 1.2 mg as a single dose at bed time. • Ophthalmic: Uveitis, iritis: 1% solution: Instill 1-2 drop(s) into the eye up to 4 times daily (adults). • Contraindications: Glaucoma, Benign prostatic hyperplasia, achalasia of esophagus, paralytic ileus, severe ulcerative colitis, intestinal ileus, severe ulcerative colitis, intestinal atony, obstructive uropathy, myasthenia gravis, CHF with tachycardia. Atropine Brand names: Atro Injection, Atrosulph, Atropine. Atropine Poisoning/ Belladonna Poisoning Atropine/ belladonna poisoning may occur due to drug overdose or consumption of seeds and berries of belladonna/datura plant. Symptoms of poisoning are: Dry mouth, difficulty in swallowing and talking, dry, flushed and hot skin, fever, urinary retention, decreased bowel sounds, a scarlet rash may appear, dilated pupil (mydriasis), photophobia, blurring of near vision, hypotension, weak and rapid pulse. The central effects include restlessness, confusion, psychotic behaviour, weakness, muscle in-coordination, hallucinations, convulsions, and coma. Finally cardiovascular collapse with respiratory depression and failure. Treatment Treatment should be started in a dark quiet room to relieve photophobia. Treatment includes gastric lavage, universal antidote, anticholinesterase such as physostigmine / neostigmine and other general measures such appropriate. MCQs 1. Which one of the following is not the therapeutic use of atropine? (a) As a mydriatic (b) As an antidote for organophosphate poisoning (c) As a preanaesthetic medication (d) As an anti-inflammatory agent 2. Atropine sulphate, a parasympatholytic drug belongs to the class _____. (a) Amino alcohol esters (b) Amino alkyl ethers (c) Amino alcohols (d) Amino amides To proceed with the TEST ON ATROPINE,

* Do not miss the test on this topic on the TEST PACKAGES page. This blog prepares you for GPAT RRB Pharmacist Recruitment Exam Common Recruitment Examination for AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE D.Pharm, B.Pharm, and Pharm.D. Exams Cholinergic Receptors: • The receptors which respond to Acetylcholine are cholinergic receptors. These receptors are found in central and peripheral nervous system. • There are two main types of cholinergic receptors: Nicotinic and Muscarinic receptors. Nicotinic Receptors • Nicotinic receptors are directly linked to ligand gated ion channels. • They are selectively activated by nicotine and blocked by tubocurarine or hexamethonium. • On the basis of location and selectivity, nicotinic receptors are divided into two types; I) N1 or Nm: These receptors are present at skeletal muscle endplate and mediate skeletal muscle contractions. They are selectively stimulated by phenyltrimethyl ammonium and are blocked by tubocurarine. II) N2 or Nn: These are present in ganglionic cells, adrenal medullary cells, in spinal cord and in certain areas of brain. In CNS Ach plays a significant role in memory, arousal and analgesia through Nn receptors. Muscarinic Receptors • The Muscarinic receptors are named such because they are responsive to muscarine (a natural alkaloid). • Muscarinic receptors are metabotropic i.e. G-protein coupled receptors. • There are five types of Muscarinic receptors: M1, M2, M3, M4 and M5. M1 Receptors: o M1 is Gq protein - coupled receptor. o It has + ve effect. It stimulates the target organ. o M1 is generally found in two specific locations: CNS where it is involved in memory, arousal and analgesia and parietal cells (gastric glands) where it increases the stomach acid. o It also increases endocrine gland secretions such as increase in the saliva. o M1 receptors work via phospholipase C, increasing IP3 and DAG levels. M2 Receptors: o M2 receptors are cardiac muscarinic receptors. o M2 receptors are Gi protein - coupled receptors. o They have –ve effect. o They are inhibitory; hyperpolarizing membranes by increasing potassium conductance.M2 is mainly going to target two different places: one is the heart (SA node, AV node and bundle of his) and the other is presynaptic membrane. o M2 receptor at presynaptic membrane inhibits the further release of Ach. o M2 receptors increase heart parasympathetic effects and there will be decrease in the chromotropy, inotropy and dromotropy of the heart. M3 Receptors: o M3 receptors are glandular muscarinic receptors o They are found on exocrine glands, smooth muscles, ciliary muscles and pupil of the eye. o M3 is Gq protein - coupled receptor. o It has + ve effect. M4 & M5 Receptors: o M4 and M5 receptors are predominantly found in the CNS. They play role in memory, arousal and analgesia. o M4 receptors act through Gi protein to inhibit adenylate cyclase. They also function by a direct regulatory action on K+ and Ca2+ion channels. When M4 receptors in tracheal smooth muscle stimulated, they inhibit the release of Ach same as that of M2 receptors do. o M5 receptors may regulate dopamine release at terminals within the striatum. • SAR of Ach reveals that a cationic ammonium group is essential for muscarinic as well as nicotinic receptor activities. • Acetylcholine (agonist) and atropine (antagonist) compete with each other at muscarinic receptors. MCQs 1. Identify a wrong statement about cholinergic receptors. a) These receptors respond to Acetylcholine. b) They are found in ANS only. c) Nicotinic receptors are directly linked to ligand gated ion channels. d) M2 receptors are cardiac muscarinic receptors. 2. All of the following statements about nicotinic receptors are correct, except: a) Nm receptors are present at skeletal muscle endplate. b) Nn receptors are present in ganglionic cells. c) Nicotinic receptors are selectively activated by hexamethonium. d) Nicotinic receptors are found in central and peripheral nervous system. To proceed with the TEST ON CHOLINERGIC RECEPTORS,

GPAT Preparation RRB Pharmacist Recruitment Exam Common Recruitment Examination AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Preparation Drugs Controller Exams Preparation DPEE D.Pharm, B.Pharm, and Pharm.D. notes • Acetylcholine is a neurotransmitter. • Acetylcholine plays a crucial role in both the central nervous system (CNS) and the peripheral nervous system (PNS). In the PNS, it functions in both the voluntary (somatic) and involuntary (autonomic) nervous systems. • Acetylcholine is synthesized locally in the cholinergic nerve endings. • In cholinergic cells, an acetyl group is transferred from acetyl-coenzyme A (CoA) to choline to synthesize Ach. This reaction is catalyzed by the enzyme choline acetyltransferase (ChAT). • Choline acetyltransferase (ChAT) is synthesized in the rough endoplasmic reticulum of all cholinergic cells. • Acetylcholine is an ester of acetic acid and choline. • Acetylcholine is hygroscopic in nature and is water soluble. • Storage condition: As it is hygroscopic in nature, it should be stored in air-tight dry container in a cool place. • SAR of Acetylcholine (Ach) (See image): 1) SAR of Ach reveals that a cationic ammonium group is essential for muscarinic as well as nicotinic receptor activities. 2) If one or more of the methyl groups on nitrogen atom are replaced by hydrogen or ethyl group, both muscarinic as well as nicotinic receptor activities are reduced. 3) Only compounds possessing a positive charge on the atom in the position of the nitrogen has appreciable muscarinic activity. 4) The muscarinic agonist should have an oxygen atom, preferably ester-like oxygen, capable of participating in a hydrogen bond. 5) There should be no more than five atoms between the nitrogen and the terminal hydrogen atom for maximal muscarinic potency. This rule is known as Ings rule of five. 6) When the methyl groups are replaced by three ethyl groups, the resulting compound is a cholinergic antagonist. • There are two main types of receptors for acetylcholine: Nicotinic and Muscarinic receptors. • Nicotinic receptors are ligand gated ion channels. • Muscarinic receptors are primarily referred to as G protein coupled receptors (GPCR). • Pharmacological Actions of Cholinergic Drugs: In general, pharmacological actions of cholinergic drugs are 1. Decrease in heart rate, force of contraction and electrical conductivity in heart i.e negative chronotropic, negative inotropic and negative dromotropic effects on the heart respectively. 2. Hypotension 3. Increase in gastric motility 4. Micturition (urinary bladder) 5. Increase salivary secretion 6. Increase bronchial secretions and cause bronchospasm 7. Increase sweating 8. Miosis and reduction in intraocular tension (eye) 9. Spasm of accommodation (eye) 10. In CNS Ach plays a significant role in memory, arousal and analgesia through Nn receptors. • Cholinesterase is the enzyme that metablises ACh. Cholinesterases are of two types: 1) True cholinesterase i.e. Acetylcholinesterase is found primarily in the blood on red blood cell membranes, in neuromuscular junctions, and in other neural synapses. 2) Pseudo-cholinesterases i.e. Butyrylcholinesterase is produced in the liver and found primarily in blood plasma. • Neuromuscular-blocking agents block the action of acetylcholine at the neuromuscular junction (NMJ), thereby causing paralysis of the affected skeletal muscles. These agents are Nicotinic receptor blockers. • According to Cholinergic hypothesis, Alzheimers disease (AD) is caused due to reduced synthesis of acetylcholine. • Ach is used to induce miosis during ocular surgery. It has limited therapeutic uses because a considerable amount of it is destroyed immediately by pseudo cholinesterases in plasma and by true cholinesterase at the site of receptors. • Miochol-E is a brand name of Ach. It is acetylcholine chloride intraocular solution used to constrict the pupil of the eye during cataract surgery or other types of eye surgery. MCQs 1) In acetylcholine, replacement of one or more of the methyl groups on nitrogen atom by hydrogen or ethyl group a) Increases both muscarinic and nicotinic activity b) Decreases both muscarinic and nicotinic activity c) Increases the muscarinic activity d) Increases the nicotinic activity 2) What is wrong about acetylcholine? (a) It is an ester of acetic acid and choline. (b) It has positively charge carbon in its structure. (c) It is hygroscopic in nature. (d) It is water soluble. 3) Effect of acetylcholine on heart is ______. (a) positive chronotropic (b) negative chronotropic (c) positive inotropic (d) positive dromotropic 4) Neuromuscular-blocking agents block the action of ______ at the neuromuscular junction. (a) acetylcholine (b) histamine (c) adrenaline (d) noradrenaline 5) Which neurotransmitter is significantly reduced in the brain of Alzheimers patient? a) Acetylcholine b) Serotonin c) Dopamine d) GABA To proceed with the TEST ON ACETYLCHOLINE for GPAT under the GPAT category,
The Graduate Pharmacy Aptitude Test (GPAT) is not just an examination; it is a gateway to a world of opportunities for aspiring pharmacists in India. Conducted annually by the National Board of Examinations in Medical Sciences (NBEMS) on behalf of the Pharmacy Council of India (PCI), GPAT serves as a crucial benchmark for assessing the knowledge and skills of pharmacy graduates. Over the years, it has evolved into a key assessment tool for evaluating the academic and professional readiness of students aspiring to pursue advanced education or careers in pharmacy. Conducted annually, GPAT serves as a gateway for admission into leading institutions like the National Institute of Pharmaceutical Education and Research (NIPER). The exam has witnessed a steady rise in popularity, with thousands of candidates appearing each year to compete for opportunities in academia, industry, and research. But why should pharmacy students prioritize GPAT preparation? Here is an in-depth look at the significance of GPAT and how it can shape your career in pharmacy.

One of the most esteemed and impactful careers in the pharmacy field is that of a Drugs Inspector. These professionals work under state governments, the central government, and organizations like the Central Drugs Standard Control Organization (CDSCO). Their primary role is to ensure safe and high-quality medicines are accessible to citizens by monitoring the production, distribution, and sale of pharmaceuticals. They are responsible for enforcing the Drugs and Cosmetics Act, 1940, and other relevant laws.
फार्मसी क्षेत्रातील एक अत्यंत प्रतिष्ठित आणि प्रभावशाली करिअर म्हणजे ड्रग इन्स्पेक्टर (औषध निरीक्षक). ड्रग इन्स्पेक्टर हे राज्य सरकार, केंद्रीय सरकार, आणि CDSCO (Central Drugs Standard Control Organization) अंतर्गत कार्यरत असतात. ते औषध उत्पादन, वितरण, आणि विक्री यावर नजर ठेवून नागरिकांना सुरक्षित आणि गुणवत्तापूर्ण औषधे उपलब्ध करून देण्यासाठी काम करतात. त्यांची मुख्य जबाबदारी औषध आणि सौंदर्य प्रसाधने अधिनियम, 1940आणि इतर संबंधित कायद्यांची अंमलबजावणी करणे ही असते.
RRB Pharmacist Recruitment Exam Common Recruitment Examination AIIMS Pharmacist GPAT 2025 KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE D.Pharm, B.Pharm, and Pharm.D. MCQs 1) Potassium permanganate occurs in the form of ______. (a) dark purple coloured crystals (b) white coloured crystals (c) blue coloured crystals (d) colourless powder 2) Hydrogen peroxide is ______. (a) Colourless liquid (b) Yellow coloured gas (c) White crystalline powder (d) White amorphous powder 3) pKa of boric acid is ______. (a) 3.3 (b) 7.5 (c) 9.19 (d) 10.5 4) Boric acid behaves as a strong acid when it is dissolved in ______. (a) Water (b) Glycerine (c) Alcohol (d) Olive oil 5) Kaolin is ______. (a) Hydrated aluminium silicate (b) Magnesium trisilicate hydrate (c) Hydrated magnesium silicate (d) Hydrated magnesium carbonate Find your answers in the description below: Properties of Important Inorganic Pharmaceuticals 1. Kaolin: It is hydrated aluminium silicate. It is a soft white or yellowish white powder, odourless with clay like taste. It is insoluble in water, in mineral acids and in solutions of alkali hydroxides. Chemically, it is inert. 2. Silver nitrate: (i) It is colourless, odourless crystalline powder with bitter and metallic taste. (ii) It is soluble in water and alcohol. (iii) It is incompatible with halides like Cl−, Br−, I−, and organic compounds, tannins etc. 3. Chlorhexidine gluconate: It is a cationic biguanide compound with antimicrobial properties. 4. Hydrogen peroxide: Physical properties: (i) It is colourless, odourless, transparent liquid. (ii) It has slight astringent and acidic taste. (iii) It is miscible with water, alcohol and ether having a weakly acidic reaction. Chemical properties: (i) It is an oxidizing agent. (ii) It oxidizes potassium iodide to iodine and potassium bromide to bromine in acidic medium. (iiii) Its dilute solution has bleaching action. 5. Borax: It effloresces in dry air. It has sweetish alkaline taste. 6. Boric acid: (i) Boric acid forms glyceroboric acid complex with glycerin which acts as a strong monobasic acid. This is why glycerin is used in the assay of boric acid. (ii) Its pKa is around 9.19. (iii) It is a white, crystalline powder or colourless shiny plates unctuous to the touch or white crystals; odourless with slightly acidic and bitter taste. (iv) It is sparingly soluble in water. 7. Chlorinated lime (Bleaching powder): (I) It is a dull white powder. It has characteristic strong odour of chlorine. (ii) On exposure to air it absorbs moisture and decomposes by liberating chlorine. (iii) It is sparingly soluble in water and insoluble in alcohol. 8. Potassium permanganate: It occurs as dark purple coloured monoclinic prisms, almost opaque with a blue metallic luster. It is odourless. An aqueous solution has sweetish astringent taste. It is a powerful oxidizing agent. 9. Sodium fluoride: It is a white crystalline powder. It is odourless and soluble in water and insoluble in alcohol. 10. Carbon dioxide: (i) It is a colourless, odourless gas with faintly acidic taste, (ii) It is soluble in water, (iii) It does not support combustion (iv) CO2 when passed in water forms carbonic acid. 25. Check your Answers: 1) a) 2) d) 3) c) 4) c) 5) c)

RRB Pharmacist Recruitment Exam Common Recruitment Examination AIIMS Pharmacist GPAT KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE D.Pharm, B.Pharm, and Pharm.D. Properties of Important Inorganic Pharmaceuticals 1. Ferrous sulphate: It is odourless, bluish-green crystalline powder. It effloresces in dry air. It has astringent or metallic taste. 2. Carbonyl iron: It appears as a gray powder made up of spherical microparticles. 3. Aluminium hydroxide gel: It is the suspension of hydrated Al2O3 (aluminium oxide). Its pH is 5.5 to 8.0. Small amounts of clear liquid may separate from it on standing. 4. Magnesium hydroxide: It is white amorphous powder, odourless and tasteless, insoluble in water. 5. Magaldrate: Chemically, magaldrate is a combination of aluminum and magnesium hydroxide. 6. Sodium bicarbonate: It is colourless, crystalline powder. Odourless with saline taste. Soluble in water and insoluble in alcohol. 7. Calcium carbonate: (i) It is a fine, white, microcrystalline powder. (ii) It is odourless, tasteless and stable in air. (iii) It is insoluble in water and alcohol. (iv) It dissolves with effervescence in most common dilute acids like acetic acid, dilute HCl. 8. Hydrochloric acid: (i) It is a colourless fuming liquid with pungent odour. (ii) It is miscible with water, alcohol. (iii) Its specific gravity is 1.18. (iv) It gets oxidized by strong oxidizing agents liberating chlorine gas. 9. Ammonium chloride: It has saline taste. It is slightly hygroscopic, soluble in water, sparingly soluble in alcohol but freely soluble in glycerine. It sublimes on heating. 10. Bismuth subcarbonate: (i) It is a white or pale yellowish white tasteless powder. (ii) It is stable in air, but is affected by light. (iii) It is insoluble in water and alcohol, but dissolves with effervescence in HCl or HNO3. (iv) When ignited, it decomposes into yellow bismuth trioxide. To be continued in tomorrow’s blog......... MCQs 1) All of the following statements about Aluminium hydroxide gel are correct, EXCEPT: (a) It is the suspension of hydrated Al2O3 (aluminium oxide) (b) Its pH is 5.5 to 8.0 (c) Small amounts of clear liquid may separate from it on standing (d) Its category is antiseptic and disinfectant 2) Which one of the following compounds is a combination of aluminum and magnesium hydroxide? (a) Alumina (b) Magaldrate (c) Simethicone (d) Ferumoxytol 3) Specific gravity of Hydrochloric acid is ______. (a) 1.0 (b) 1.18 (c) 2.0 (d) 2.18 4) Which of the following compounds dissolves with effervescence in HCl or HNO3? (a) Ammonium chloride (b) Sodium fluoride (c) Bismuth subcarbonate (d) Ferrous sulphate 5) What is wrong about Ammonium chloride? (a) It has saline taste (b) It sublimes on heating (c) It is insoluble in water (d) All of the above options are correct Check your answers below: Blog content and MCQs have been taken from the following: 1) Essential Pharmacy Review for Drugs Inspector Exams by Nirali Prakashan, Pune To know more about the book:
Dear Pharmacist/ Pharmacy Student If your dream is to become a Drugs Inspector or Govt. Pharmacist or to qualify GPAT then you should understand basics in pharmacy as explained in this online class.

Dear Pharmacist/ Pharmacy Student If your dream is to become a Drugs Inspector or Govt. Pharmacist or to qualify GPAT then you should understand basics in pharmacy as explained in the class.

Applications of Artificial Intelligence in Pharmacy Artificial Intelligence (AI) is revolutionizing numerous industries, and the field of pharmacy is no exception. From drug discovery to personalized medicine, AI is transforming the way pharmacists, researchers, and healthcare providers approach patient care and pharmaceutical innovation. Let’s explore some key applications of AI in pharmacy. 1. Drug Discovery and Development AI has significantly accelerated the drug discovery process, reducing the time and cost involved in bringing new medicines to market. Machine learning algorithms analyze vast datasets to identify potential drug candidates, predict their efficacy, and simulate their interactions with biological systems. This has led to breakthroughs in treatments for diseases such as cancer and rare genetic disorders. 2. Personalized Medicine Personalized medicine tailors treatments to individual patients based on their genetic makeup, lifestyle, and medical history. AI algorithms process genomic data to predict how patients will respond to specific drugs, enabling more effective and targeted therapies. 3. Pharmacy Operations and Supply Chain Management AI optimizes pharmacy workflows and supply chain logistics, ensuring that medications are available when and where they are needed. Predictive analytics helps in demand forecasting, inventory management, and identifying supply chain disruptions. 4. Clinical Decision Support Systems (CDSS) AI-powered CDSS assist pharmacists and clinicians in making informed decisions by analyzing patient data, identifying potential drug interactions, and recommending appropriate therapies. 5. Adverse Drug Reaction (ADR) Monitoring Pharmacovigilance is a critical area where AI excels. Natural Language Processing (NLP) algorithms analyze patient records, social media, and adverse event reports to detect patterns and identify potential safety concerns. 6. Medication Adherence and Patient Engagement AI-powered mobile apps and wearable devices help patients adhere to their medication regimens by providing reminders, tracking usage, and offering real-time feedback. 7. Drug Repurposing AI identifies new uses for existing drugs by analyzing data from clinical trials, research papers, and patient records. This has been particularly useful during health crises like the COVID-19 pandemic.

First Year - D.Pharm, B.Pharm, and Pharm.D. GPAT RRB Pharmacist Recruitment Exam Common Recruitment Examination AIIMS Pharmacist KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE Uses of Important Inorganic Pharmaceuticals (Continue from the last blog) 15. Magnesium trisilicate: Non-systemic (non-absorbable) antacid; gastrointestinal protective agent with colloidal silica. 16. Silver nitrate: Bactericidal, bacteriostatic, caustic, astringent, wet dressing on burned areas, opthalmic infection. 17. Chlorhexidine gluconate: Antiseptic and mouth wash. 18. Hydrogen peroxide: As mild antiseptic, disinfectant, cleansing agent for cuts and wounds and for loosening ear wax, 1.6% solution is used in deodorants, gargles and mouth washes. As antidote in phosphorus and cyanide poisoning. As bleaching agent. 19. Boric acid: It is used in preparation of buffer solution. Antiseptic boric acid solutions are used mainly as eye and mouth wash. It is used as an ingredient in dusting powder. 20. Borax: Used as germicidal, bacteriostatic agent. It is used in preparations of eye wash, mouth washes and gargles. It is used as food preservative. It is used in cosmetic preparations as emulsifier. 21. Calamine: It has a mild astringent action. It is used in the form of dusting powder due to its soothing and protective property. 22. Chlorinated lime (Bleaching powder): It is used as disinfectant, to disinfect faeces, urine, sputum and other organic material, employed for disinfecting drainages. It is a powerful bleaching agent. It is used as one to two grams per litre for sterilization of water. 23. Potassium permanganate: Anti-infective, antiseptic and antibacterial. Antidote in barbiturate poisoning. As oxidizing agent. 1 : 5000, 1 : 15,000 solutions is used in cleaning wounds and ulcers. 24. Sodium fluoride: It is used as anticaries agent. 25. Carbon dioxide: It is used as a respiratory stimulant. It is used in treatment of drug addiction and carbon monoxide poisoning. Dry ice is used in minor surgical operation for destroying tissue. CO2 inhalation releases persistent hiccups. 26. Nitrous oxide: General anaesthesia. 27. Oxygen: O2 mixed with 5-7% CO2 is used as respiratory stimulant. 28. Ammonium carbonate: As respiratory stimulant and expectorant. 29. Antimony potassium tartrate: Emetic. 30. Barium sulphate: As contrast medium for X-rays examination of the alimentary tract. To be continued in tomorrow’s blog......... MCQs 1) Select astringent from the following. (a) Kaolin (b) Silver nitrate (c) Hydrogen peroxide (d) Charcoal 2) Which of the following compounds is used as antimicrobial agent ______. (a) Hydrogen peroxide (b) Talc (c) Calamine (d) Titanum dioxide 3) ______ are used as anticaries agent. (a) Chlorides (b) Bromodes (c) Iodides (d) Fluorides 4) Which one of the following gas produces anaesthesia with analgesia? (a) Oxygen (b) Nitrous oxide (c) Carbon dioxide (d) Ammonia 5) Potassium permangnate is a ______. (a) strong reducing agent (b) strong oxidizing agent (c) complexing agent (d) precipitating agent Check your answers below: Blog content and MCQs have been taken from the following books: 1) Essential Pharmacy Review for Drugs Inspector Exams by Nirali Prakashan, Pune To know more about the book:

RRB Pharmacist Recruitment Exam Common Recruitment Examination AIIMS Pharmacist GPAT KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE D.Pharm, B.Pharm, and Pharm.D. Uses of Important Inorganic Pharmaceuticals 1. Ferrous sulphate: Haematinic and used to treat anaemia. 2. Ferrous ascorbate: Haematinic and used to treat anaemia. 3. Carbonyl iron: Haematinic and used to treat anaemia. 4. Aluminium hydroxide gel: Non-systemic (non-absorbable) antacid, as antidiarrhoeal in cholera, externally as mild astringent and dusting powder. It shows antacid property not by neutralization but by physical adsorption of acid molecules. 5. Magaldrate: Antacid 6. Sodium bicarbonate: Systemic antacid, alkalizing agent to combat systemic acidosis, an electrolyte replenisher, an ingredient of effervescent powder. 7. Calcium carbonate: Non-systemic (non-absorbable) antacid; as a good cleaning and polishing agent used in dentifrices. 8. Hydrochloric acid: Acidifying agent 9. Ammonium chloride: Acidifying agent to treat achlorhydria, expectorant, diuretic, systemic acidifier (treatment of metabolic alkalosis) and in the treatment of urinary tract infections. 10. Bismuth subcarbonate: As antidiarroheal by protective-adsorbent mechanism; as antacid, mild astringent and antiseptic; as a topical protective in lotions and ointments. 11. Kaolin: As antidiarrhoeal and dusting powder. 12. Magnesium sulphate: As laxative; as antidote in heavy metal poisoning. 13. Magnesium trisilicate: Non-systemic (non-absorbable) antacid; gastrointestinal protective agent with colloidal silica. 14. Sodium potassium tartrate: As cathartics To be continued in tomorrow’s blog......... MCQs 1) Iron plays an important role in treatment of ______. (a) Anemia (b) Scurvy (c) Gout (d) Arthritis 2) The condition of absence of hydrochloric acid in the stomach is called ______. (a) Anemia (b) Hyperacidity (c) Rickettsia (d) Achlorhydria 3) Which one of the following agents can be used as cleansing agent in dental products? (a) Calcium gluconate (b) Sodium fluoride (c) Calcium carbonate (d) KMnO4 4) Select a haematinic compound among the followings: (a) Calcium gluconate (b) Sodium fluoride (c) Ferrous ascorbate (d) Magaldrate 5) Aluminium hydroxide gel is used in the treatment of ______. (a) Dental caries (b) Diarrhoea (c) Peptic ulcer (d) Achlorhydria Check your answers below: Blog content and MCQs have been sourced from the following: 1) Essential Pharmacy Review for Drugs Inspector Exams by Nirali Prakashan, Pune To know more about the book:

AIIMS Pharmacist Common Recruitment Examination (CRE) * Date of uploading of Detail Advertisement & Commencement of online registration of application: Start date: 07.01.2025 Close On: 31.01.2025 * Date of Examination: 26th February 2025 – 28th February 2025 To download the advertisement:

Intramolecular and Intermolecular forces for RRB Pharmacist Recruitment Exam GPAT KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE D.Pharm, B.Pharm, and Pharm.D. • Intramolecular forces hold atoms together within a molecule. Ex: Ionic bond, covalent bond, metallic bond. • Intermolecular forces exist between molecules. Ex: Dipole-dipole interactions, hydrogen bonding, London dispersion forces/ van der Waal forces. • Covalent bond results from the sharing of an electron pair between two atoms. • Sigma bond (σ bond) is a covalent bond resulting from the formation of a molecular orbital by the end-to-end overlap of atomic orbitals, denoted by the symbol σ. • Pi bond (π bond) is a covalent bond resulting from the formation of a molecular orbital by side-to-side overlap of atomic orbitals along a plane perpendicular to a line connecting the nuclei of the atoms, denoted by the symbol π. • Ionic bond is formed by the complete transfer of valence electron(s) between atoms. Ex: NaCl. • A dipole is a separation of opposite electrical charges. • Van der Waals forces are weak intermolecular forces that arise from interactions between uncharged atoms or molecules. These forces are the sum of the attractive and repulsive electrical forces between atoms and molecules. Types of Van der Waals forces include weak London Dispersion Forces and stronger dipole-dipole forces. • Dipole-dipole interactions occur when the partially positively charged part of a molecule interacts with the partially negatively charged part of the neighboring molecule. Ex: HCl. ( H+δ- Cl-δ…..H+δ- Cl-δ……. H+δ- Cl-δ) • London dispersion force is the weak intermolecular force that results from the motion of electrons that creates temporary dipoles in molecules. • Ion-dipole interaction is the result of an electrostatic interaction between a charged ion and a molecule that has a dipole. • Hydrogen bonding is a special kind of dipole-dipole interaction that occurs between a hydrogen atom covalently bonded to a highly electronegative atom (such as nitrogen, oxygen, or fluorine) and an electronegative atom in a different molecule or within the same molecule. The partially positive end of the hydrogen atom is attracted to the partially negative end of the electronegative atom. While nitrogen (N), oxygen (O), and fluorine (F) are the primary atoms involved in hydrogen bonding, chlorine (Cl) can participate in hydrogen bonding under certain conditions. To be continued in tomorrow’s blog: MCQs 1) Which of the following is an example of an intramolecular force? a) Hydrogen bonding b) Dipole-dipole interaction c) Covalent bond d) London dispersion forces 2) What causes London dispersion forces? a) Permanent dipoles b) Temporary dipoles due to electron movement c) Covalent bonding d) Ionic bonding 3) Which of the following compounds exhibits hydrogen bonding? a) CH4 b) H2O c) CO2 d) CCl4 4) Which force is responsible for the high boiling point of water? a) Ionic bond b) Covalent bond c) Hydrogen bonding d) London dispersion forces 5) Why do molecules with strong intermolecular forces have higher boiling points? a) They have more atoms b) They require more energy to separate c) They are heavier d) They are less polar Check your answers below: Recommended book for the preparation of GPAT and Drugs Inspector Exams, "ESSENTIAL PHARMACY REVIEW FOR DRUGS INSPECTOR EXAMS", NIRALI PRAKASHAN, PUNE To know more about the book:

Basics of Pharmaceutical Organic Chemistry and MCQs related to them for RRB Pharmacist Recruitment Exam GPAT KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams DPEE D.Pharm, B.Pharm, and Pharm.D. • Isomers are molecules with the same molecular formula (i.e. the same number of atoms of each element), but different structural or spatial arrangements of the atoms within the molecule. • Tautomerism is a type of isomerism which involves simple proton transfer in an intramolecular fashion. Ex: Keto-enol tautomerism, enamine-imine tautomerism, lactam-lactim tautomerism, etc. • Stereochemistry is the branch of chemistry concerned with the three-dimensional arrangement of atoms and molecules and the effect of this on chemical reactions. • Stereoisomers are the compounds that have same molecular formula and the same connectivity, but different arrangement of the atoms in 3-dimensional space. • Conformational isomers are the stereoisomers that have different spatial arrangement of its atoms and groups that arise due to the rotation of a part of the molecule about a single bond. These are non-isolable and are easily interconvertible. • Configurational isomers are the stereoisomers that have different spatial arrangement of atoms and groups about a rigid part of a molecule i.e about a double bond or ring or asymmetric center. Configurational isomers are isolable and are not easily interconvertible. Interconversions of these isomers involve bond breaking and bond reforming process. • Optical isomers: These are the compounds having the same molecular and structural formula but differ only in their action towards plane polarized light or optical activity. Optical isomers are enantiomers. • Stereogenic center or stereocenter or chiral center is an atom (usually carbon) within a molecule that has four different groups or atoms attached to it. • A racemic mixture is a 50/50 combination of two enantiomers (commonly referred to as levo and dextro enantiomers) of a chiral compound, resulting in optical inactivity due to the cancellation of their individual optical activities. • The R and S configuration system is a method for describing the three-dimensional arrangement of substituents around a chiral center in a molecule. The system was introduced by Cahn, Ingold, and Prelog. To be continued in tomorrow’s blog: MCQs 1) The following statements are given: [P] Conformational isomers are interconvertible by rotation around a single bond while configurational isomers cannot be interconverted without breaking a bond. [Q] Configurational isomers and conformational isomers could be optically active or optically inactive, depending on the circumstances [R] Geometric isomers must have a double bond in their structures [S] Geometric and optical isomers are the two distinct categories of configurational isomers. Choose the correct combination of statements. (a) P, Q & S are true while R is false (b) P, R & S are true while Q is false (c) Q, R & S are true while P is false (d) P, Q & R are true while S is false 2) Optically active compounds _____. (a) Can rotate plane of polarized light (b) Cannot rotate plane of polarized light (c) Can increase rate of a chemical reaction (d) Can prevent oxidation of compounds 3) Asymmetric carbon is a carbon that has _____. (a) At least two different groups or atoms attached to it (b) At least two same groups or atoms attached to it (c) Four same groups or atoms attached to it (d) Four different groups or atoms attached to it 4) The isomerism exhibited by compounds that have the same molecular formula but differ in their spatial arrangement is (a) Structural isomerism (b) Geometric isomerism (c) Stereoisomerism (d) Conformational isomerism 5) Which of the following is a chiral molecule? (a) 2-butanol (b) Ethanol (c) 1,2-dichloroethane (d) Benzene Check your answers below: Recommended book for the preparation of GPAT and Drugs Inspector Exams, "ESSENTIAL PHARMACY REVIEW FOR DRUGS INSPECTOR EXAMS", NIRALI PRAKASHAN, PUNE To know more about the book:

Pharmacists in India have a wide array of Government Job Opportunities across various sectors, offering stable and rewarding careers with significant social impact. Here is an overview of key positions available: Central Government Opportunities: • Drugs Inspector and Drugs Controller: Recruited by the Central Drugs Standard Control Organization (CDSCO) and Union Public Service Commission (UPSC). • Research Positions (Scientists): Available in organizations like the Central Drug Research Institute (CDRI), Indian Council of Medical Research (ICMR), Defence Research and Development Organisation (DRDO), etc. • Academic Roles: Positions as professors in central government academic and research institutes. • Pharmacists in Central Government Hospitals: Opportunities in hospitals such as All India Institute of Medical Sciences (AIIMS), Safdarjung Hospital, etc. • Indian Railways: Pharmacist positions through the Railway Recruitment Board (RRB). • Central Government Health Scheme (CGHS): Employs pharmacists to manage dispensaries in major cities. • Employee State Insurance Corporation (ESIC): Offers pharmacist roles in their healthcare facilities. • Armed Forces and Paramilitary Services: Positions include Pharmacist in Indian Air Force as Airmen (Med Asst) Trade, Pharmacist in Indian Army as Sepoy (Pharma), Pharmacist in Assam Rifles, Assistant Sub Inspector (Pharmacist) in Indo-Tibetan Border Police (ITBP), and roles in Border Security Force (BSF). • Indian Space Research Organisation (ISRO): Pharmacist positions in healthcare facilities of ISRO. • Public Sector Undertakings (PSUs): Opportunities in pharmaceutical PSUs like Indian Drugs and Pharmaceuticals Limited (IDPL), Hindustan Antibiotics Limited (HAL), Karnataka Antibiotics and Pharmaceuticals Limited (KAPL), Bengal Chemicals and Pharmaceuticals Limited (BCPL), and Rajasthan Drugs and Pharmaceuticals Limited (RDPL), as well as other PSUs with healthcare facilities. • National Health Mission (NHM): Pharmacist roles in various health programs. • Staff Selection Commission (SSC): Recruitment for Pharmacist Grade II positions. • Delhi Subordinate Services Selection Board (DSSSB): Pharmacist recruitment for Delhi government services. State Government Opportunities: • State Drug Control Departments: Positions like Drugs Inspector and Assistant Drugs Controller. For instance, the Food and Drug Administration (FDA) in Maharashtra is expected to announce over 400 Drugs Inspector posts soon. • Academic Roles: Professorships in state government academic and research institutes. • State Government Hospitals: Pharmacist positions in various state-run hospitals. • Directorate of Health Services (DHS): Pharmacist recruitment in states like Maharashtra. • Directorate of Medical Education & Research (DMER): Pharmacist recruitment in states like Maharashtra. • Arogya Vibhag Bharti: Pharmacy Officer positions in Maharashtra. Local Bodies: • Zilla Parishad: Pharmacist recruitment in district councils. • Municipal Corporations: Pharmacist positions in urban local bodies. Educational Qualifications, Experience, and Age Limit: • These criteria vary depending on the specific position and recruiting agency and are notified in official recruitment notifications. Benefits of Government Jobs for Pharmacists: • Job Security: Government positions offer excellent stability. • Social Impact: Contribute to public health and community service. • Competitive Salaries and Benefits: Attractive pay packages, pension plans, and other perks. • Growth Opportunities: Prospects for career advancement and professional development. Preparation Tips for Aspiring Candidates: • Thorough Preparation: Study and revise relevant concepts diligently and practice MCQs thoroughly. • Stay Updated: Keep abreast of the latest drug information, regulations, and government notifications. • General Knowledge and Reasoning: Enhance skills in these areas, as they are often part of the examination process. • Practice Mock Tests: Regularly take mock tests to assess preparation and improve performance. For comprehensive preparation, consider utilizing resources like "Essential Pharmacy Review for Drugs Inspector Exams", and "Pharmacist Recruitment Exam", books published by Nirali Prakashan, Pune. These books offer extensive multiple-choice questions (MCQs) and key points for efficient revision. Note: Always verify the authenticity of any job posting and be cautious of potential scams. Refer to official government websites and trusted sources for accurate information.
Basics of Pharmaceutical Organic Chemistry and MCQs related to them for RRB Pharmacist Recruitment Exam KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams GPAT DPEE D.Pharm, B.Pharm, and Pharm.D. 1. An orbit is a well-defined circular path followed by electron around nucleus. 2. Atomic orbitals are regions of space around the nucleus of an atom where an electron is likely to be found. 3. Electronic configuration is the arrangement of electrons in the orbitals of an atom or molecule. 4. Hybridization is the concept of mixing atomic orbitals to form new hybrid orbitals which are equivalent (same in energy). 5. Chemical bond refers to the forces of attraction holding atoms together to form molecules. 6. Bond fission is the breaking of chemical bonds. 7. Free radicals are uncharged molecules or atoms having an unpaired valence electron. They are typically highly reactive and short-lived. 8. Bond energy (E) is the amount of energy required to break apart a mole of molecules into its component atoms. It is a measure of the strength of a chemical bond. 9. Chemical reaction is a process in which one or more substances (the reactants) are converted to one or more different substances, (the products). It involves bond breaking and bond making. 10. Energy of activation (Ea) is the minimum energy required to start a chemical reaction. The activation energy of a reaction is usually denoted by Ea and is expressed as kilojoules per mole (kJ/mol) or rarely kilocalories per mole (kcal/mol). To be continued in tomorrow’s blog........ MCQs 1) The minimum energy required to initiate a chemical reaction is _____ a) Bond energy b) Fission energy c) Energy of activation d) Energy of reaction 2) Uncharged molecules or atoms having an unpaired valence electron are ___ a) ions b) free radicals c) uncharged ions d) energetic ions 3) Atomic orbitals are regions of space where _____ a) electrons are likely to be found. b) protons are likely to be found. c) neutrons are likely to be found. d) electrical charges are likely to be found. 4) Hybridization is the concept of_____ a) mixing atomic orbitals b) mixing atomic orbits c) mixing atomic charges d) demixing atomic orbitals 5) A measure of the strength of a chemical bond is ____ a) energy of activation b) bond energy c) exothermic energy d) endothermic energy Check your answers below:
Ten Important Concepts from Pharmaceutical Jurisprudence and Pharmacy Law and Ethics and MCQs related to them for RRB Pharmacist Recruitment Exam KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams GPAT DPEE D.Pharm, B.Pharm, and Pharm.D. 1. Registered pharmacist: Means a person whose name for the time being is entered in the register of the pharmacists of the state in which he is for the time being residing or carrying on his profession or business of pharmacy. 2. New Drug: (I) A new substance of chemical, biological or biotechnological origin in bulk or prepared dosage form used for prevention, diagnosis, or treatment of disease in man or animals, which except during local clinical trials has not been used in the country to any significant extent and has not been recognised as effective and safe by the licensing authority; OR (II) A drug already approved by the Licensing Authority (CDSCO) for certain claims, which is now proposed to be marketed with modified or new claims namely indications dosage, dosage form; OR (III) A fixed dose combination of two or more drugs individually approved earlier for certain claims which are now proposed to be combined for the first time in a ratio; OR (IV) The ratio of ingredients in an already marketed combination is proposed to be changed with certain claims; OR (V) A modified or sustained release form of a drug or novel drug delivery system of any drug approved by the Central Licencing Authority; OR (VI) A vaccine, recombinant Deoxyribonucleic Acid (r-DNA) derived product, living modified organism, monoclonal antibody, stem cell derived product, gene therapeutic product or xenografts, intended to be used as drug. (Note: Points (V) and (VI) in the above description of New Drug are as per given in the New Drugs and Clinical Trials Rules, 2019). 3. Misbranded drug: A drug shall be deemed to be misbranded if: (I) it is so colored, coated, powdered or polished that, damage is concealed; OR (II) it is made to appear of better or greater therapeutic value than it really is; OR (III) it is not labeled in the prescribed manner; OR (IV) its label or container or anything accompanying the drugs bears any statement, design or device which makes any false claim for the drug or which is false or misleading in any particular. 4. Adulterated drug: A drug shall be deemed to be adulterated if: (I) it consists, in whole or in part, of any filthy, putrid or decomposed substance; OR (II) it has been prepared, packed or stored under insanitary conditions whereby it may have been contaminated with filth or whereby it may have been rendered injurious to health; OR (III) its container is composed in whole or in part, of any poisonous or deleterious substance which may render the contents injurious to health; OR (IV) it bears or contains, a colour other than prescribed which may be used for the purpose of colouring only; OR (V) it contains any harmful or toxic substance which may render it injurious to health; OR (VI) any substance mixed with it so as to reduce its quality or strength. 5. Spurious drug: A drug shall be deemed to be spurious if: (I) it is imported under a name which belongs to another drug; OR (II) It is an imitation of, or a substitute for, another drug or resembles another drug in a manner likely to deceive or bears upon it or upon its label or container the name of another drug unless it is plainly and conspicuously marked so as to reveal its true character and its lack of identity with such other drug; OR (III) the label or the container bears the name of an individual or company purporting to be the manufacturer of the drug, which individual or company is fictitious or does not exist; OR (IV) it has been substituted wholly or in part by another drug or substance; OR (V) it purports to be the product of a manufacturer of whom it is not truly a product. 6. Illicit traffic in relation to narcotic drugs and psychotropic substances: (i) Cultivating any coca plant or gathering any portion of coca plant; (ii) Cultivating the opium poppy or any cannabis plant; (iii) Engaging in the production, manufacture, possession, sale, purchase, transportation, warehousing, concealment, use or consumption, import inter-state, export inter-state, import into India, export from India or transhipment, of narcotic drugs or psychotropic substances; (iv) Handling or letting out any premises for the carrying on of any of the activities referred to in sub-clauses above, other than those permitted under this Act. It also includes: I. Financing, directly or indirectly, any of the afore-mentioned activities; II. Abetting or conspiring in the furtherance of or in support of doing any of the afore-mentioned activities; and III. Harbouring persons engaged in any of the afore-mentioned activities. 7. Magic remedy: It includes a talisman, mantra, kavacha, and any other charm of any kind which is alleged to possess miraculous powers for or in the diagnosis, cure, mitigation, treatment or prevention of any disease in human beings or animals or for affecting or influencing in any way the structure or any organic function of the body of human beings or animals. 8. Animal: Any living creature other than a human being. (Prevention of Cruelty to Animals Act, 1960) 9. Ceiling price: A price fixed by the Government for Scheduled formulations in accordance with the provisions of this Order (DPCO, 2013). 10. Clinical trial: Clinical trial in relation to a new drug or investigational new drug means any systematic study of such new drug or investigational new drug in human subjects to generate data for discovering or verifying its (i) clinical or; (ii) pharmacological including pharmacodynamics, pharmacokinetics or; (iii) adverse effects, with the objective of determining the safety, efficacy or tolerance of such new drug or investigational new drug. MCQs 1. If a drug contains a colour which is not prescribed is called ______. (a) Misbranded (b) Spurious drug (c) Adulterated drug (d) New drug 2. If a product purporting to be the product of a manufacturer of whom its not true product means a substance is ______. (a) Adulterated (b) Spurious (c) Misbranded (d) Deterioated 3. The drug which is clinically not recognized safe by the licensing authority is known as ______. (a) Imported drug (b) Patented drug (c) Misbranded drug (d) New drug 4. As per the definition in Prevention of Cruelty to Animals Act, 1960 Animal means any living creature EXCEPT: (a) Microorganisms (b) Butterflies (c) Human beings (d) Insects 5. Magic remedies include ______. (a) Modern medicines (b) Ayurvedic medicines (c) Homeopathic medicines (d) Mantras and Kavachas 6. Any drug described as filthy, putrid or decomposed substance in whole or in part is termed as ___. (a) substandard drug (b) spurious drug (c) adulterated drug (d) misbranded drug 7. A label of drug that is not in prescribed manner is known as ______. (a) Misbranded (b) Spurious (c) Adulterated (d) New Drug 8. What is Ceiling Price? (a) Maximum price fixed by government on Scheduled formulations (b) Maximum price fixed by government on Non-Scheduled formulations (c) Minimum price fixed by government on Scheduled formulations (d) Maximum price fixed by the manufacturer Check your answers below:

Scope and Objectives of Various Legislations in Pharmaceutical Jurisprudence and Pharmacy Law and Ethics and MCQs related to them for RRB Pharmacist Recruitment Exam KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams GPAT DPEE D.Pharm, B.Pharm, and Pharm.D. • Scope and Objectives of Various Legislations 1. Drugs and Cosmetics Act, 1940 and Rules 1945: To regulate the manufacture, distribution, sale and import of the drugs and cosmetics. 2. Pharmacy Act, 1948 and Rules: (I) To control and regulate pharmacy profession in India. (II) To raise the status of pharmacy profession in India. 3. Drugs and Magic Remedies (Objectionable Advertisement) Act, 1954: (I) To control certain types of advertisements related to drugs. (II) To prohibit certain types of advertisements related to magic remedies. 4. Narcotic Drugs and Psychotropic Substances Act, 1985 and Rules (NDPS Act 1985): (I) To consolidate and amend the laws relating to narcotic drugs and psychotropic substances. (II) To make stringent provisions for control and regulation of operations to narcotic drugs and psychotropic substances. (III) To prevent illicit traffic in N.D.P.S. 5. Medical Termination of Pregnancy Act, 1971: To provide for the termination of certain pregnancies by registered medical practitioners and for matters connected therewith or incidental thereto. 6. Poisons Act, 1919: To control and regulate sale, possession, possession for sale and import of poisons. 7. Prevention of Cruelty to Animals Act, 1960: To prevent the infliction of unnecessary pain or suffering on animals. 8. The Patents Act, 1970: (I) To encourage inventors to make a greater contribution to their field by granting them exclusive rights to their inventions. (II) To speed the development of an indigenous pharmaceutical industry and to guarantee that Indian public had access to low-cost drugs. 9. The Food Safety and Standards Act, 2006: (I) To consolidate the laws relating to food (II) to establish the Food Safety and Standards Authority of India (FSSAI) for laying down science based standards for articles of food and to regulate their manufacture, storage, distribution, sale and import, to ensure availability of safe and wholesome food for human consumption and for matters connected therewith or incidental thereto. 10. Consumer Protection Act, 2019: Protection of the interests of consumers and for the said purpose, to establish authorities for timely and effective administration and settlement of consumers disputes and for matters connected therewith or incidental thereto. 11. Disaster Management Act, 2005: Effective management of disasters and for matters connected therewith or incidental thereto. 12. Drugs Price Control Order (DPCO) 2013: (I) To control production, supply, distribution, etc. of essential medicines for maintaining or increasing supplies and for securing their equitable distribution and availability at fair prices. 13. New Drugs and Clinical Trials Rules, 2019: To promote clinical research in India. 14. Clinical Establishments (Registration and Regulation) Act, 2010: (I) To provide for the registration and regulation of clinical establishments in India. (II) To prescribe minimum standards of facilities and services for all categories of health care establishments (except teaching hospitals). (III) To establish a digital registry of Clinical Establishments at National, State and District level. (IV) To prevent quackery by unqualified practitioners by introducing registration system. 15. Biomedical Waste Management Rules, 2016: To improve the collection, segregation, processing, treatment and disposal of bio-medical wastes in an environmentally sound management thereby, reducing the bio-medical waste generation and its impact on the environment. MCQs 1. The main objective of ______ is to regulate the profession and practice of pharmacy and to raise the status of profession of pharmacy in India. (a) D and C Act, 1940 (b) Pharmacy Act, 1948 (c) UGC Act, 1956 (d) AICTE Act, 1987 2. To promote clinical research in India is the objective of (a) Clinical Establishment Act and Rules (b) Drugs and Cosmetics Act 1940 and Rules 1945 (c) Pharmacy Act-1948 and Rules (d) New Drugs and Clinical Trials Rules, 2019. 3. Which one of the following is not the objective of NDPS Act, 1985? (a) To control certain types of advertisements related to drugs. (b) To consolidate and amend the laws relating to narcotic drugs and psychotropic substances. (c) To make stringent provisions for control and regulation of operations to narcotic drugs and psychotropic substances. (d) To prevent illicit traffic in N.D.P.S. 4. The Act enacted to prevent quackery by unqualified practitioners is ______. (a) Consumer Protection Act (b) The Food Safety and Standards Act, 2006 (c) Drugs and Magic Remedies (Objectionable Advertisement) Act 1954 (d) Clinical Establishments (Registration and Regulation) Act, 2010 5. To regulate the manufacture, distribution, sale and import of the drugs and cosmetics is the objective of _______. (a) Drugs Price Control Order (DPCO) 2013 (b) Drugs and Cosmetics Act 1940 and Rules 1945 (c) Pharmacy Act-1948 and Rules (d) Consumer Protection Act 6. The rules prescribed for reducing the bio-medical waste generation and its impact on the environment are called as _______. (a) Biomedical Water Management Rules, 2006 (b) Biomedicine Waste Management Rules, 2016 (c) Biomedical Waste Management Rules, 2016 (d) Biomaterial Waste Management Rules, 2006 7. An objective of Disaster Management Act is ______. (a) Effective management of disasters due to COVID 19 (b) Effective management of diseases (c) Effective management of disasters due to pandemics (d) Effective management of disasters 8. To encourage inventors to make a greater contribution to their field by granting them exclusive rights to their inventions is an objective of ______. (a) The Copyrights Act, 1957 (b) The Patents Act, 1970 (c) The Designs Act, 2000 (d) Trade and Merchandise Act 1958 Check your answers below:

Schedules from D & C Act, 1940 and MCQs for RRB Pharmacist Recruitment Exam KGMU Pharmacist Recruitment Exam KSSSCI Pharmacist Recruitment Exam MPESB Pharmacist Recruitment Exam Drugs Inspector Exams Drugs Controller Exams GPAT DPEE D.Pharm, B.Pharm, and Pharm.D. Schedules and Description J: List of diseases and ailments which a drug may not purport to prevent or cure or make claims to prevent or cure. E.g., AIDS, Appendicitis, Bronchial Asthma, Cataract, Paralysis, etc. K: Classes of drugs which are exempted from certain provisions applicable to manufacture and sale of drugs. M: GMP was first incorporated in Schedule M of the Drugs and Cosmetics Rules, 1945 in the year 1988 Good manufacturing practices and requirements of premises, plant and equipment for pharmaceutical products: Part 1 : Good manufacturing practices for premises and materials. Part 1A : Specific requirements for manufacture of sterile products, parenteral preparations (small volume injectables and large volume parenterals) and sterile ophthalmic preparations. Part 1B : Specific requirements for manufacture of oral solid dosage forms (tablets and capsules). Part 1C : Specific requirements for manufacture of oral liquids (syrups, elixirs, emulsions and suspensions). Part 1D : Specific requirements for manufacture of topical products, i.e. external preparations (creams, ointments, pastes, emulsions, lotions, solutions, dusting powders and identical products). Part 1E : Specific requirements for manufacture of metered-dose-inhalers (MDI). Part 1F : Specific requirements of premises, plant and materials for manufacture of active pharmaceutical ingredients (bulk drugs). Part 2 : Requirements of plant and equipment. M-I: Good manufacturing practices and requirements of premises, plant and equipment for homeopathic medicines. M-II: Requirements of factory premises for manufacture of cosmetics. M-III: Quality management system for notified medical devices and in-vitro diagnostics. N: List of minimum equipment for the efficient running of a pharmacy. O: Standard for disinfectant fluids. Part 1 : Provision applicable to black fluids and white fluids. Part 2 : Provisions applicable to other disinfectant fluids. P: Life period of drugs. Condition of storage: 1. The term “cold place” means a place having a temperature not exceeding 8oC. 2. The term “cool place” means a place having a temperature between 10oC and 25oC. 3. Capsules should be kept in a well-closed container at temperature not exceeding 30oC. 4. Wherever condition of storage is not specified, it may be stored under normal room temperature. P1: Pack sizes of drugs. Q: Part 1 : List of dyes, colours and pigments permitted to be used in cosmetics and soaps. Part 2 : List of colours permitted to be used in soaps. R: Standards for condoms made of rubber latex intended for single use and other mechanical contraceptives. R1: Standards for medical devices. The medical devices conform to the Indian Standards laid down from time to time by the Bureau of Indian Standards. S: Standards for cosmetics in finished form. T: Good manufacturing practices for Ayurvedic, Siddha and Unani medicines. U: Particulars to be shown in manufacturing and analytical records. Records of raw materials. U(I): Particulars to be shown in the manufacturing records and records of raw materials of cosmetics. V: Standards for patent or proprietary medicines. X: List of psychotropic substances. Warning: To be sold by retail on the prescription of a Registered Medical Practitioner only. E.g. Amphetamine, etc. Y: Requirements and guidelines for permission to import and / or manufacture of new drugs for sale or to undertake clinical trials. MCQs 1. GMP requirement of factory premises, plants and equipment ______. (a) Schedule - M (b) Schedule - P (c) Schedule - Q (d) Schedule – S 2. Requirements for efficient running of pharmacy prescribed under which Schedule? (a) Sch. M (b) Sch. N (c) Sch. H (d) Sch. W 3. Given the following are schedule X drugs, except ______. (a) Amobarbital (b) Amphetamine (c) Glutethimide (d) Phenformin 4. Sch. R(1) Stands for ______. (a) Standards for mechanical contraceptives (b) Standards for medical devices. (c) Standards for ophthalmic preparations. (d) Standards for cosmetic 5. Schedule ‘C’ and Schedule ‘N’ as per the Drugs and Cosmetics Act deal with the following: (P) Standards for cosmetics (Q) Biological and special products (R) Life period of drugs (S) List of minimum equipments for the efficient running of a pharmacy Identify the correct statements. (a) P, Q (b) Q, S (c) R, S (d) P, R 6. List of diseases and ailments which a drug may not purport to prevent or cure or make claims to prevent or cure under the Drugs and Cosmetics Rule 1945 is given under ______. (a) Schedule J (b) Schedule K (c) Schedule M (d) Schedule P 7. Standards for condoms made of rubber latex intended for single use and other mechanical contraceptives are provided in ______. (a) Schedule F (b) Schedule G (c) Schedule P (d) Schedule R 8. As per schedule P Carbenicillin Sodium Powder should be stored in/at ______. (a) A cool place (b) A cold place (c) Temperature not exceeding 5°C (d) Well closed container, protect from light, in cool place, protect from light Check your answers below:

Schedules from D & C Act, 1940 and MCQs for RRB, KGMU, KSSSCI, MPESB Pharmacist Exams / GPAT / DPEE / Drugs Inspector Exams / D.Pharm, B.Pharm, and Pharm.D. Schedules and Description A: Forms for various purposes such as applications for licenses, granting licenses, sending memorandum, issuing certificate of test or analysis, etc. C: Biological and special products E.g., Sera, vaccines for parenteral injections, ophthalmic preparations, etc. C (1): Other special products such as antibiotics and preparations thereof not in a form to be administered parenterally, etc. F (PART XII B): Requirements for the functioning and operation of a blood bank and/or for preparation of blood components. F (PART XII C): (I) Requirements for manufacture of blood products. (II) Requirements for manufacture of blood products from bulk finished products. F (PART XII D): Requirements for collection, processing, testing, storage, banking and release of umbilical cord blood derived stem cells. F (PART XIII): General. F(I): Part I : Provisions applicable to the production of vaccines. Part II : Antisera (Provisions applicable to the production of all Sera from Living Animals). Part III : Diagnostic Antigens (Provisions applicable to the manufacture and standardization of diagnostic agents (bacterial origin)). Part IV : General. F (II): Standards for surgical dressings. F (III): Standards for umbilical tapes. FF: Standards for ophthalmic preparations. G: List of drugs to be taken under the supervision of registered medical practitioner only. E.g., Insulin, etc. H: Prescription Drugs: To be sold by retail only on the prescription of registered medical practitioner only. H1: List of drugs not to be sold by retail without the prescription of a Registered Medical Practitioner. The supply of these drugs is required to be recorded at the time of supply in a prescription register specially maintained for the purpose and the serial number of the entry in the register shall be entered on the prescription. E.g., Diazepam, Tramadol, etc. MCQs 1. Schedule FF is prescribed for ______. (a) Life period of drugs (b) Pack size of drug (c) Standards of cosmetics (d) Standards of ophthalmic preparations 2. Diazepam is an example of following schedule. (a) Sch. N (b) Sch. Q (c) Sch. H1 (d) Sch. G 3. Metformin is an example of following schedule. (a) Sch. G (b) Sch. X (c) Sch. H (d) Sch. H-1 4. List of substances required to be taken only under supervision of a Registered Medical Practitioner covers under ______. (a) Schedule G (b) Schedule H (c) Schedule I (d) Schedule J 5. Pro-forma for sending memorandum is included in which schedule? (a) D (b) A (c) FF (d) Q 6. Vaccines and Sera are included in of D and C Act. (a) Schedule C (b) Schedule G (c) Schedule FF (d) Schedule X 7. Drug sold under the prescription of registered medical practitioner comes under: (a) Schedule G (b) Schedule H (c) Schedule I (d) Schedule J 8. Biological and Biotechnological products are included in schedule ______. (a) A (b) B (c) C and C1 (d) X Check your answers below:

Advertisement No.: Admin-11011(13)/2/2024-eoffice Dated: 29-12-2024 * Additional Drugs Controller * Joint Drugs Controller * Deputy Drugs Controller
Pharmacodynamics concepts for RRB, KGMU, KSSSCI, MPESB Pharmacist Exams / GPAT / DPEE / Drugs Inspector Exams / D.Pharm, B.Pharm, and Pharm.D. o Placebo and nocebo effects. Nocebo is negative thoughts evoked by the pessimistic attitude of the patient. Placebo is opposite of nocebo. o Drug Tolerance: It is a phenomenon where a drug becomes ineffective upon its repeated administration at the usual therapeutic dose. Progressive increase in the dose is required to produce the desired therapeutic effect. o Drug dependence (neuroadaptation): It is an altered physiological state in which the user has a strong desire to continue taking the drug either to experience its effect or to avoid the discomfort of its absence. Examples of drugs producing dependence are opioids, barbiturates, alcohol and benzodiazepines. o Combined effects of drugs: When two or more drugs are given simultaneously or in quick succession, they may not affect action of each other, or they may exhibit additive effect or synergism or antagonism. o Additive effect: The desirable therapeutic effect of the two or more drugs is in the same direction and simply adds up: Effect of drugs A + B = effect of drug A + effect of drug B. E.g. Ephedrine + Aminophylline as bronchodilator; Aspirin + Paracetamol as analgesic - antipyretic o Synergistic effect: The desirable therapeutic effect of combination of two or more drugs is greater than the sum of their individual effects: Effect of drug A + B > effect of drug A + effect of drug B. E.g. Cotrimoxazole (sulphamethoxazole + trimethoprim) as bactericidal; Codeine and aspirin as analgesics; Procaine and adrenaline combination increases the duration of action of procaine. o Antagonism: The phenomenon where one drug decreases or stops the action of another drug then it is said to be antagonism. Effect of drugs A + B < effect of drug A + effect of drug B o Depending on the mechanism involved, antagonism may be: 1. Chemical Antagonism: The two drugs react chemically and form a pharmacologically inactive or undesirable product. E.g. KMnO4 oxidizes alkaloids. It is used for gastric lavage in poisoning. Chelating agents (BAL, calcium disodium edetate) form complex with toxic metals (As, Pb). Drugs may react when mixed in the same syringe or infusion bottle and form undesirable products. E.g. Thiopentone sodium + succinylcholine chloride; Penicillin-G sodium + succinylcholine chloride 2. Physical antagonism: Antagonism due to physical property of antagonist. E.g., Activated charcoal adsorbs alkaloids and can prevent their absorption, used in alkaloidal poisonings. 3. Receptor antagonism: One drug is receptor antagonist. It blocks the receptor action of the other drug which is agonist. Receptor antagonism can be competitive or non-competitive. (a) Competitive (reversible) antagonism: The antagonist competes with the agonist for the same receptors. This antagonism can be reversed by increasing concentration of the agonist at the receptor site. E.g. Acetylcholine (agonist) and atropine (antagonist) compete with each other at muscarinic receptors. (b) Non-competitive (irreversible) antagonism: The antagonist binds to an allosteric site and inactivates the receptor so that the agonist cannot be bound effectively. This antagonism cannot be reversed by increasing concentration of the agonist at the receptor site. E.g. Phenoxybenzamine binds irreversibly to α-adrenergic receptors; antagonism between diazepam – bicuculline is also non-competitive. 4. Physiological Antagonism: The two drugs act on different receptors or by different mechanisms, and have exactly opposite pharmacological effects. E.g., Bronchoconstriction produced by histamine in anaphylactic shock is antagonized by adrenaline; effect of glucagon and insulin on blood sugar level is antagonistic. o Therapeutic Index (Safety Margin): It is defined as the ratio of median lethal dose to median effective dose. A drug with larger therapeutic index is safer than one with smaller therapeutic index. Hence, drug with lesser therapeutic index should be administered cautiously. MCQs 1. In the presence of this type of antagonist, antagonism cannot be overcome by increasing agonist concentrations. (a) Competitive (b) Noncompetitive (c) Reversible (d) Nonspecific 2. When the total pharmacological effect of two or more drugs administered together is equal to the sum of their individual pharmacological actions, the effect is called (a) Synergism (b) Additive effect (c) Antagonism (d) Adverse effect 3. The ratio of median lethal dose to median effective dose is _____. (a) Bioavailability of a drug (b) Therapeutic index (c) Apparent volume of distribution of a drug (d) Therapeutic window 4. The phenomenon where interaction between two or more drugs produces an effect greater than the sum of their individual effects is _____. (a) Additive effect (b) Synergism (c) Antagonism (d) None of these 5. Identify the correct statement. (a) A drug with larger therapeutic index is safer than with one smaller therapeutic index (b) A drug with larger therapeutic index is more toxic than one with smaller therapeutic index. (c) Therapeutic index is not associated with safety of drugs. (d) Therapeutic index shows the potency of a drug 6. The opposite action of two drugs on the same physiological system is called as _____. (a) Synergism (b) Antagonism (c) Drug tolerance (d) Drug dependence 7. ED50 is the dose of a _____. (a) test substance that produces desirable effects in 50% of the animals in a dose group (b) test substance that kills 50% of the animals in a dose group (c) substance that produces maximum effect in 50% of the animals in a dose group (d) substance that produces maximum adverse effects in 50% of the animals in a dose group 8. Insulin and glucagon are considered (a) Pharmacological antagonist (b) Physiological antagonists (c) Pharmacodynamic antagonist (d) Chemical antagonist Check your answers below:

Pharmacodynamics for RRB, KGMU, KSSSCI, MPESB Pharmacist Exams / GPAT / DPEE / Drugs Inspector Exams / D.Pharm, B.Pharm, and Pharm.D. o Pharmacodynamics is the study of biochemical and physiological effects of drugs and their mechanisms of action. o Pharmacodynamics deals with the relationship between concentration of drug at the site of action and the magnitude of the effect produced by the drug. o Pharmacodynamics deals with what a drug does to the body. o The basic types of drug action can be classified as: 1. Stimulation 2. Depression 3. Irritation 4. Replacement 5. Cytotoxic action 1. Stimulation refers to increase in the activity of specialized cells, e.g. epinephrine stimulates heart, caffeine stimulates CNS. 2. Depression means decrease in activity of specialized cells, e.g. diazepam depresses CNS, propranolol depresses heart. 3. Irritation suggests a non-selective, harmful effect and is particularly applied to less specialized cells (epithelium, connective tissue). 4. Replacement refers to the use of electrolytes, vitamins, hormones or their congeners in deficiency states e.g. iron preparations in iron deficiency anaemia, insulin in diabetes mellitus, vitamin C in Scurvy, etc. 5. Cytotoxic action refers to toxic to living cells, e.g. penicillin, chloroquine, fluorouracil, cyclophosphamide, etc. o General Mechanisms of Drug Action include 1. Physicochemical properties and drug action, e.g., (i) Due to oxidizing property, potassium permanganate acts as an antiseptic. (ii) Antacids like sodium bicarbonate neutralizes gastric HCl. 2. Drug interaction with a discrete target biomolecules like enzymes, ion channels, transporters, receptors, nucleic acids, structural proteins, etc. o Ligand is any molecule which attaches selectively to a particular receptor. o Agonist is an agent which stimulates a receptor to produce an effect similar to that of the physiological signal molecule. o Inverse agonist is an agent which stimulates a receptor to produce an effect opposite to that of the agonist. o Antagonist is an agent which prevents the action of an agonist on a receptor. o Partial agonist: It is an agent which stimulates a receptor to produce submaximal effect but antagonizes the action of a full agonist. o Factors modifying action of drug are: Body size, Age, Sex, Genetics, Route of administration, Environmental factors and time of administration, Psychological factor, Pathological states (Presence of disease), Cumulation, Drug Tolerance, Drug dependence (neuroadaptation), Combined effects of drugs. o Tachyphylaxis (acute tolerance): It is the rapid development of tolerance when the drug is administered repeatedly at very short intervals of time. E.g., repeated administration of ephedrine in the treatment of asthma may produce tolerance to it. MCQs 1. An agent which activates a receptor to produce an effect similar to that of the physiological signal molecule is (a) Antagonist (b) Agonist (c) Inverse agonist (d) Enzyme 2. Study of what the drug does to the body is _____. (a) Pharmacokinetics (b) Pharmacodynamics (c) Biopharmaceutics (d) Pharmacology 3. Identify the wrong option: Pharmacodynamics is the study of _____. (a) Effects of drugs (b) Mechanism of drug action (c) Drug-drug interaction (d) Safety of drug 4. The initial combination of the drug with its receptor resulting in a conformational change in the latter is known as _____. (a) Drug action (b) Drug effect (c) Drug affinity (d) Synergism 5. Tachyphylaxis is _____. (a) Acute drug tolerance (b) Increase heart rate (c) Movement of white blood cells (d) Allergic reactions 6. The study of the relationship between drug concentration and its effects is _______. (a) Pharmacokinetics (b) Pharmacodynamics (c) Pharmacotherapeutics (d) Pharmacovigilance 7. What does the term “Potentiation” mean? (a) Cumulative ability of a drug (b) Hypersensitivity to a drug (c) Fast tolerance developing (d) Intensive increase of drug effects due to their combination 8. Rapid development of tolerance on repeated doses of a drug in quick succession, with reduction in clinical response, is termed as ________ (a) synergism (b) antagonism (c) idiosyncrasy (d) tachyphylaxis Check your answers below:

ADVERTISEMENT FOR RECRUITMENT RALLY AIRMEN (MED ASST) TRADE INCLUDING PHARMACIST INTAKE 02/2025. Indian Air Force offers opportunities for MALE INDIAN / GORKHA (A SUBJECT OF NEPAL) CITIZENS from States of Tamil Nadu, Kerala, Karnataka, Telangana, Andhra Pradesh and UTs of Puducherry & Lakshadweep to join the IAF as Airmen in the Group ‘Y’, Medical Assistant trade. The Recruitment Test will be held at Maharaja’s College Ground, PT Usha Road, Shenoys, Ernakulam, Kochi, Kerala-682011. To download the advertisement:

Uttarakhand Medical Service Selection Board तिथि विस्तार नोटिस- फार्मासिस्ट (भेषज) परीक्षा- 2024 (चिकित्सा शिक्षा विभागान्तर्गत) Date of Notice 16th December 2024 To download the notice –
Multi-compartment Models and Non-linear pharmacokinetics for RRB, KGMU, KSSSCI, MPESB Pharmacist Exams / GPAT / DPEE / Drugs Inspector Exams / D.Pharm, B.Pharm, and Pharm.D. • Multicompartment Models are also known as Delayed Distribution Models. • Loading (Priming) Dose (XL): It is defined as the amount of an initial dose of a certain drug needed to reach a target plasma concentration. • The loading dose (LD) where the target concentration is Css is calculated by the formula LD = V X Css Where, V = Apparent volume of distribution and Css = Steady state plasma concentration of the drug • Maintenance Dose (XM) is defined as the dose needed to maintain the concentration within the therapeutic window (Css) when given repeatedly at a constant interval. • Problems: 1. What is a loading dose of drug A (V = 20L, oral bioavailability = 40%, target plasma concentration = 5 mg/l)? Sol. Loading dose (XL) = Css.av X (V/F) XL = 5 mg/L X (20L / 0.40) = 250 mg 2. What is the maintenance dose (XM) of drug A for plasma level of 5 mg/L, TID, p.o. Cl is 7.5 L/h, F is 75%? Sol. Maintenance dose (XM) = Css,av X Cl (total) X dosing interval, (T) / F TID i.e. three times a day i.e. dosing interval (T) = 8hrs XM = 5 mg/L X 7.5 L/h X 8 hrs / 0.75 = 400 mg. 3. What is the I.V. loading dose to give a serum theophylline concentration of 12 mg/L in a 60 kg man? (V for theophylline is 0.7 L/kg) Sol. Loading dose (XL) = Css.av X V XL = (12 mg/L) (0.7 L/kg) (60 kg) = 504 mg • The elimination rate constant is the rate at which drug is removed from the body assuming first-order elimination. It is often represented by K or KE. Its unit is time^-1 i.e. 1/time. (Note: Here ^ indicates raised to the power of). • Steady State / Plateau Principle: Steady-state (plateau) conditions are attained when the rate of drug entering the system (dose per unit time) equals the rate of drug exiting the system and no further drug accumulation occurs. • In practice, during a repeat-dose regimen, steady state is assumed to be reached in 5 half-lives unless dose interval is very much longer than t½. The time taken to reach steady-state does not depend on dose size, dosing interval and number of doses. • Linear pharmacokinetics always exhibits linear relation between dose (single or multiple doses) and plasma concentration of a drug i.e. in a given interval always the same drug fraction is eliminated. • For a drug exhibiting linear kinetics all semilog plots of C (concentration) versus t(time) for different doses when corrected for dose administered, are superimposable. This is called principle of superposition. • Non-linear pharmacokinetics shows a mixture of first-order and zero-order rate processes and the pharmacokinetic parameters change with the size of the dose administered. • The non-linear pharmacokinetic behaviour is also called as dose-dependent, mixed-order, and capacity-limited kinetics. • Non-linear or dose-dependent pharmacokinetics can be described by Michaelis-Menten equation as: − dC / dt = Vmax C / Km + C where, − dC / dt = Rate of decrease of drug concentration with time, Vmax = Maximum rate of the process, Km = Michaelis-Menten constant (drug concentration at which the rate of process is 50% of Vmax) and C = Drug concentration in the body • Example: The elimination rate of a drug with a concentration 0.8 µg/mL, Km of 0.1 mg/mL and a Vmax of 0.5 mg/mL per hour As per above Equation Solution: Elimination rate = Vmax C / Km + C = (0.5 X 0.8) / (0.1 + 0.8) = 0.4/0.9 = 0.444 µg/mL/h. • Dosage regimen is the decision of drug administration regarding formulation, route of administration, drug dose, dosing interval and treatment duration. MCQs 1. Regarding two compartment pharmacokinetics all are true EXCEPT: (a) a drug is always removed from the peripheral compartment. (b) a drug with a high volume of distribution is likely to be lipophilic. (c) a drug can have a short duration of action while being eliminated very slowly. (d) most anaesthetic drugs are modelled well with a two-compartment model. 2. Time required to reach the steady state after a dosage regimen depends on ______. (a) Route of administration (b) Half life of a drug (c) Dosage interval (d) Dose of drug 3. The loading dose of a drug is usually based on ______. (a) Total body clearance of the drug (b) Percentage of drug bound to plasma protein (c) Fraction of drug excreted unchanged in urine (d) Apparent volume of distribution and desired drug concentration in plasma 4. Non-linear pharmacokinetics is also known as _______. (a) dose dependent (b) enzyme capacity limited (c) saturation pharmacokinetics (d) All of the above 5. The characteristic of non-linear pharmacokinetics include _______. (a) Area under the curve is proportional to the dose (b) Elimination half-life remains constant (c) Area under the curve is not proportional to the dose (d) Amount of drug excreted through remains constant 6. Which of following drug shows non-linearity in hepatic excretion? (a) Carbamazepine (b) Propranolol (c) Penicillin (d) Thiopental 7. Drugs that show nonlinear pharmacokinetics have which of the following property? (a) A constant ratio of drug metabolites is formed as the administered dose increases. (b) The elimination half- life increases as the administered dose increases. (c) The area under the plasma drug concentration versus time curve increases in direct proportion to an increase in the administered dose. (d) Both low and high doses follow first -order elimination kinetics. 8. Which of the following statements about Km, the Michaelis constant in Michaelis-Menten kinetics is correct? (a) is defined as the concentration of substrate required for the reaction to reach maximum velocity. (b) is defined as the dissociation constant of the enzyme-substrate complex. (c) is expressed in terms of the reaction velocity. (d) is a measure of the affinity the enzyme has for its substrate Check your answers below:
Drug Excretion, Clearance and Plasma Half-Life for RRB, KGMU, KSSSCI, MPESB Pharmacist Exams / GPAT / DPEE / Drugs Inspector Exams / D.Pharm, B.Pharm, and Pharm.D. o Drug excretion is the irreversible removal of drugs and/or their metabolites from the body by all possible routes of excretion. o The excretion of drugs via kidneys is known as renal excretion. Excretion via all other possible routes is known as non-renal excretion of drugs. o Depending upon the drugs pKa, changes in urine pH will change the ratio of ionised to unionised drug, affecting the rate of drug excretion. For example alkalinization of urine by the administration of Sodium bicarbonate will increase the excretion of salicylates (weak acids). o The cycle in which the drug is absorbed, secreted in bile and reabsorbed is known as enterohepatic cycling (Fig.). o Clearance is the hypothetical volume of body fluids containing drug from which the drug is removed or cleared completely in a specific period of time. Thus clearance is a measurement of drug elimination from the body. o Elimination of drug from the body involves two processes, biotransformation or drug metabolism and drug excretion. o Clearance is the second primary pharmacokinetic parameter. It is represented as Cl. Its unit is ml/min or liters/hour. It is constant for any given plasma drug concentration. o Secondary pharmacokinetic parameters are derived from primary pharmacokinetic parameters. These are half-life (t½), bioavailability, AUC, Cmax, etc. o Elimination half-life of drug i.e. time required to decrease plasma drug concentration by half, can be obtained as, t1/2 = 0.693/ K Where, K is Elimination rate constant and t1/2 is Elimination half-life. Unit of Elimination half-life is hours or minutes. o Half-life is a hybrid/secondary pharmacokinetic parameter and is determined by the apparent volume of distribution (V) and clearance (Cl). o t1/2 (min) = (0.693 X V (mL/kg)) / Cl (mL/min/kg) o Half-life is directly proportional to V and inversely proportional to Cl. MCQs 1. Total body clearance is (a) the drug elimination rate divided by the plasma drug concentration (b) the drug elimination rate divided by the Vd (c) the amount of drug in body divided by the plasma drug concentration (d) None of the above 2. Renal excretion of drug depend on (a) urine flow (b) pH of urine (c) Physicochemical properties of drug (d) All of above 3. Elimination is expressed as follows: (a) Rate of renal tubular reabsorption (b) Clearance speed of some volume of blood from substance (c) Time required to decrease the amount of drug in plasma by one-half (d) Clearance of an organism from a xenobiotic 4. Below mentioned all factors increases plasma elimination half life except (a) Higher protein binding (b) Higher tissue binding (c) Higher apparent Vd (d) Higher renal/ hepatic clearance 5. The biological half-life of drug: (a) is a constant physical property of the drug (b) is a constant chemical property of the drug (c) may be increased in patients with impaired renal failure (d) may be decreased in patients by giving the drug by rapid I.V. injection 6. The half life of a drug eliminated by first order elimination kinetics will be longer in individuals who have an: (a) increased volume of distribution or increased clearance (b) increased volume of distribution or decreased clearance (c) decreased volume of distribution or increased clearance (d) decreased volume of distribution or decreased clearance 7. Half life (t½) is the time required to: (a) change the amount of a drug in plasma by half during elimination (b) metabolize a half of an introduced drug into the active metabolite (c) absorb a half of an introduced drug (d) bind a half of an introduced drug to plasma proteins 8. Elimination rate constant (Kelim) is defined by the following parameter: (a) rate of absorption (b) maximal concentration of a substance in plasma (c) highest single dose (d) half life (t½) 9. Systemic clearance (Cl) is related with: (a) only the concentration of substances in plasma (b) only the elimination rate constant (c) volume of distribution, half life and elimination rate constant (d) bioavailability and half life 10. Biological Half life equation for first order process is (a) t1/2 = a/2K (b) t½ = 0.693/K (c) t½ = 1/aK (d) t½ = 3/2 K Check your answers below:
o Drug Metabolism: • Drug metabolism is also known as biotransformation of drugs or drug detoxification. • Drug metabolism is a process which involves transformation of drug or any foreign compound into a polar, water soluble form suitable for excretion. • Liver is the major organ for drug metabolism. • First pass effect: A first-pass effect is defined as the rapid uptake and metabolism of an agent into inactive compounds by the liver, immediately after intestinal absorption and before it reaches the systemic circulation. • Enzyme Induction: Exposure of body to some drugs results in the increase in the activity of drug metabolising enzymes. The process by which the activity of metabolising enzymes is increased is referred as Enzyme Induction. The drugs or xenobiotics which cause enzyme induction are called Enzyme Inducers. Enzyme inducers increase the rate of drug metabolism and decreases duration of drug action. Drugs which increase the activity of enzyme systems of their own metabolism are known as Auto Inducers. • Enzyme Inhibition: Enzyme Inhibition is the decrease in drug metabolising activity of an enzyme. Enzyme inhibition may occur in different ways: (i) The drug interferes with enzyme synthesis or cause degradation of enzyme. Cycloheximide, puromycin and actinomycin D interfere with protein synthesis and reduce enzyme content. Whereas, disulfiram, carbon tetrachloride and secobarbital destroy cytochrome P-450. (ii) Some drugs interact with the enzyme sites and make it unavailable for metabolism of other drug. This type of inhibition may be competitive or non-competitive. - In competitive inhibiton, structurally similar compounds compete for the same site on the enzyme. It is reversible and can be overcome by higher concentration of one of the drugs. For example, neostigmine inhibits metabolism of structurally similar drug, acetylcholine. - In non-competitive inhibition, the inhibitor inhibits the enzyme by combining at a site on the enzyme other than the active site i.e. allosteric site. This type of inhibition is irreversible and is not reverted by increasing substrate concentration. For example, isoniazid inhibits metabolism of phenytoin. Mercury, arsenic and organophosphorus insecticides cause non-competitive inhibition of enzymes. MCQs 1. Which tissue has the greatest capacity to biotransform drugs? (a) kidney (b) liver (c) lung (d) skin 2. The term “biotransformation” includes the following ______. (a) Accumulation of substances in a fat tissue (b) Binding of substances with plasma proteins (c) Accumulation of substances in a tissue (d) Process of physicochemical and biochemical alteration of a drug in the body 3. Metabolic transformation (phase 1) is ______. (a) Acetylation and methylation of substances (b) Transformation of substances due to oxidation, reduction or hydrolysis (c) Glucuronide formation (d) Binding to plasma proteins 4. Identify the correct statement. (a) First pass effect occurs in case of oral administration of drugs (b) First pass effect occurs in case of parenteral administration of drugs (c) First pass effect occurs in case of topical administration of drugs (d) First pass effect occurs in case of sublingual administration of drugs 5. The process of alteration of drugs within living organism so as to modify its activity or nature is _____. (a) Excretion (b) Metabolism (c) Absorption (d) Bioavailability 6. Phase II reactions of metabolism are also known as _____. (a) Functionalisation reactions (b) Conjugation reactions (c) Redox reactions (d) Hydrolysis reactions 7. The process in which some drugs stimulate their own metabolism is known as _____. (a) Enzyme inhibition (b) Autoinduction (c) Product inhibition (d) None of these 8. Biotransformation of drugs is to render them: (a) Less ionized (b) More pharmacologically active (c) More lipid soluble (d) Less lipid soluble 9. Tick the drug type for which microsomal oxidation is the most prominent: (a) Lipid soluble (b) Water soluble (c) Low molecular weight (d) High molecular weight 10. Pick out the right statement: (a) Microsomal oxidation always results in inactivation of a compound (b) Microsomal oxidation results in a decrease of compound toxicity (c) Microsomal oxidation results in an increase of ionization and water solubility of a drug (d) Microsomal oxidation results in an increase of lipid solubility of a drug thus its excretion from the organism is facilitated Check your answers below:

o Drug Distribution: • It is reversible transfer of drug form one location or compartment to another within the body. o Apparent Volume of Distribution (Vd): • It is defined as the volume of fluid in which drug appears to be distributed or dissolved. It is not a true anatomic or physiologic volume. o Drug-Protein Binding: •The reversible binding of drug with non-specific and non-functional sites on the body proteins without showing any biological effects is called as drug-protein binding. o Plasma Protein Binding: • It acts as temporary storage of the drug and makes the drug long acting. o Blood Brain Barrier (BBB): • The BBB is composed of a monolayer of brain capillary endothelial cells that are fused together by tight junction. Apart from tight junction, the brain micro capillaries lack fenestrations and show presence of astrocytes and pericytes on the outer surface of the endothelium. o Partition coefficient of a drug between a fat-like solvent (such as octane, chloroform, heptane) and water, may be considered as an indicator of lipid solubility. o The extent of distribution of a drug depends on its: • Lipid solubility • Ionization at physiological pH • Extent of binding to plasma and tissue proteins • Presence of tissue-specific transporters and • Tissue size and perfusion o Numerical: Drug A has pKa of 7.4 and partition coefficient of unionized form of 0.21. Drug B has pKa of 11.3 and partition coefficient of unionized form of 0.005. Both Drug A and Drug B are weak acid drugs. Predict their distribution rates in high perfused tissues and give reason. (Hint: since the partition coefficients of both drugs are small, you can assume the distribution is limited by the permeability) Solution: In the permeability limited distribution, the drug transfer takes place by passive diffusion and is affected by surface area of membrane, membrane thickness, concentration gradient, partition coefficient and ionization (FICKS law of diffusion). In this case, the rate of distribution is highly correlated to the drugs effective partition coefficient at the blood pH (~pH 7.4). Drug A has pKa of 7.4. Therefore, its fraction of unionized form is about 0.5 at pH 7.4. So its effective partition coefficient is ≈0.5*0.21≈0.1. Drug B has pKa of 11.3. Therefore its fraction of unionized form is about 1 at pH 7.4. So its effective partition coefficient is ≈1*0.005≈0.005. Effective partition coefficient of drug A > Effective partition coefficient of drug B. Hence, drug A will distribute much faster. MCQs 1. The initial distribution of a drug into tissue is determined chiefly by the (a) rate of blood flow to tissue (b) GFR (c) tissue binding (d) protein binding 2. The loading dose of a drug is based upon the (a) time taken for complete elimination (b) percentage of drug excreted unchanged in urine (c) percentage of drug bound to plasma protein (d) apparent volume of distribution and the desired drug concentration in plasma 3. The volume of distribution of drugs is: (a) An expression of total body volume (b) A measure of total fluid volume (c) A relationship between the total amount of drug in the body and the concentration of the drug in the blood (d) Proportional to bioavailability of the drug 4. Which of the following characteristics is most likely to be associated with a high apparent volume of distribution? (a) Penetration across the blood : brain and blood : testis barriers (b) Extensive binding to plasma protein (c) Distribution into total body water (d) Extensive binding to tissue constituents 5. The rate of drug transport across a cell membrane by lipid diffusion depends on all of the following EXCEPT (a) Surface area of absorption (b) Lipid partition coefficient (c) Density of transporters (d) Concentration gradient 6. Which of the following drug selectively bound to extravascular tissues? (a) Warfarin (b) Diazepam (c) Digitoxin (d) Chloroquin 7. Plasma protein binding _____ the volume of distribution of drugs. (a) increases (b) decreases (c) no change (d) none of the above 8. Following intravenous administration, drugs are distributed fastest to: (a) the skin, kidney, and brain (b) the liver, kidney, and brain (c) the liver, adipose, and brain (d) the liver, kidney, and adipose 9. _______ is the tight junctions between sertoli cells. (a) BBB (b) placental barrier (c) blood-testis barrier (d) endothelial barrier 10. If a drug is highly bound to plasma proteins, what might be its reason or consequence? (a) It is most likely carried by x-glycoprotein (b) It has a high renal clearance (c) It has a large Vd (d) It is a likely candidate for drug interaction Check your answers below:
o Bioavailability: It is defined as the rate at which, and extent (amount) to which the unchanged drug is absorbed from its dosage form and becomes available at the site of drug action. • Absolute Bioavailability (F): It is the ratio of the systemic availability of a drug administered orally (extravascular) and the systemic availability of the same drug administered intravenously. • Significance of absolute bioavailability is to characterize inherent absorption properties of a drug from extravascular site and to determine an appropriate oral dose of a drug relative to an IV dose. • Relative Bioavailability (Fr): It is defined as the extent of absorption from the test preparation of a drug relative to the extent of absorption from the reference product of the same drug. • Pharmacokinetic methods are indirect methods to assess bioavailability of a drug. • AUC (Area under the plasma drug concentration–time curve) is a measurement of the extent of drug bioavailability. o Official Dissolution Test Apparatus: • Rotating Basket Apparatus (USP - I / IP - II) • Rotating Paddle Apparatus (USP - II / IP - I) • Reciprocating Cylinder (USP - III) • Flow-Through Cell (USP -IV) • Paddle over Disk (USP - V) • Rotating Cylinder (USP - VI) • Reciprocating Holder (USP - VII) o According to USP, In-Vitro In-Vivo Correlation (IVIVC) refers to the establishment of a rational relationship between a biological property or a parameter derived from biological property produced due to dosage form and a physicochemical parameter or characteristic of the same dosage form. o Bioequivalence: Two formulations of a drug are said to be bioequivalent if the rate and extent to which the drug reaches the systemic circulation after administration of their respective formulations are statistically comparable. o Biowaiver: It is an official approval of the waiver for conducting a bioequivalence study (i.e. bioequivalence study is not considered necessary by FDA) in relation to an application for drug approval process. Due to biowaiver, unnecessary human experiments can be avoided and it saves both time and money to bring new products to market. MCQs 1. Which condition usually increases the rate of drug dissolution from tablet? a) Increase in particle size of drug b) Use of the ionized, or salt, form of the drug c) Decrease in the surface area of the drug d) Use of the free acid or free base form of the drug 2. What does the term bioavailability mean? (a) Plasma protein binding degree of substance (b) Permeability through the brain-blood barrier (c) Fraction of an unchanged drug reaching the systemic circulation following any route administration (d) Amount of a substance in urine relative to the initial dose 3. In order to determine the absolute bioavailability of a drug given as an oral extended release tablet, the bioavailability of a drug must be compared to the bioavailability of a drug from a) An immediate release oral tablet containing the same amount of the active ingredient b) A reterence (Brand) extended release tablet, i.e., a pharmaceutical equivalent c) A parenteral solution of a drug given by IV bolus or IV infusion d) An oral solution of the drug in the same dose 4. The rate of drug bioavailability is most rapid when the drug is formulated as a ______ (a) controlled released product (b) hard gelatin capsule (c) tablet (d) solution 5. Dissolution test apparatus I as per IP is ______ (a) Paddle over Disk (b) Rotating Cylinder (c) Rotating basket (d) Rotating paddle 6. USP dissolution test apparatus type-II is ______ (a) Rotating paddle apparatus (b) Paddle over disc (c) Rotating basket type (d) Flow-through cell 7. The range of absolute bioavailability is ______. (a) O% to 1% (b) O% to 100% (c) −1% to 1% (d) − 1% to 100% 8. Bioavailability differences among drugs oral formulations are most likely to occur if it ______. (a) is freely water soluble (b) is incompletely absorbed (c) is completely absorbed (d) undergoes little first-pass metabolism Check your answers below:
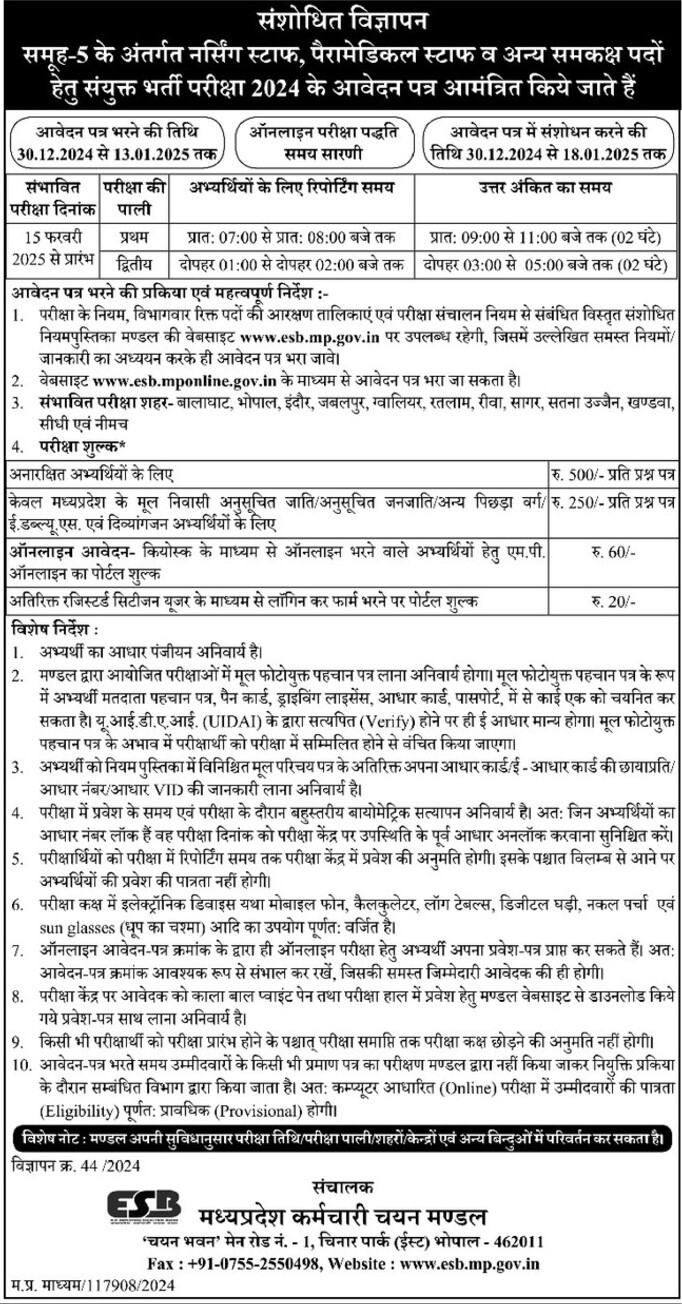
To download the detailed notification,
Pharmacokinetics includes the study of absorption, distribution, tissue or protein binding, biotransformation (metabolism) and excretion of the drug. Pharmacokinetics deals with what body does to a drug. Drug absorption is the process of movement of unchanged drug from the site of administration to the systemic circulation. • Processes/Mechanisms of drug absorption include: 1. Transcellular passive diffusion 2. Filtration or Paracellular/Pore transport/Convective transport 3. Carrier-mediated transport 4. Ion-pair transport 5. Endocytosis • Transcellular passive diffusion (Non-ionic diffusion): - The drug diffuses across the membrane in the direction of its concentration gradient i.e. from higher to lower concentration. - The cell membrane plays no active role in the process. It is the energy independent process. - The diffusion rate increases with increase in the lipid : water partition coefficient of the drug. - Majority of drugs get absorbed by this mechanism. • Filtration or Paracellular/Pore transport/Convective transport: - Filtration is passage of drugs through aqueous pores in the membrane or through paracellular spaces. - Drugs that are moderate in size and hydrophilic (water soluble) like atenolol, furosemide, cimetidine, ranitidine and famotidine (MW − 200-270) are absorbed by the paracellular route. • Carrier-mediated transport: - It involves participation of the cell membrane in the transfer of molecules. - In this process, a carrier (transporter) moves the solute (drug) molecule across the cell membrane. - Depending on requirement of energy, carrier transport is of two types: (a) Facilitated passive diffusion and (b) Active transport. • Facilitated passive diffusion: - It is a carrier-mediated process which occurs across the concentration gradient, i.e. from higher concentration to lower concentration. - It does not require energy. - Organic cation transporters OCT1, OCT2 and OCT3 are transporters causing facilitated passive diffusion. - Absorption of vitamin B12 occurs by facilitated passive diffusion. The entry of glucose into muscle and fat cells by GLUT4 is also facilitated passive diffusion. • Active transport: - In this process, carriers carry drug molecules against concentration gradient i.e. from lower concentration to higher concentration (uphill transport). - This process utilizes energy provided by adenosine triphosphate (ATP). - Endogenous substances like pyrimidines, L-amino acids, monosaccharides, sodium, potassium, iron and vitamins such as niacin, pyridoxin and ascorbic acid are transported by active transport process. - Examples of drugs absorbed by this mechanism are - methyldopa and levodopa are absorbed by Lamino acid transport system; 5-fluorouracil and 5-bromouracil are absorbed via pyrimidine transport system. • Ion-pair transport: - In this mechanism, a charged molecule forms a reversible complex with an oppositely charged molecule, thus a neutral ion-pair complex is formed. - This neutral ion-pair complex has sufficient lipophilicity as well as aqueous solubility and passes through the membrane by passive diffusion. - After absorption the complex dissociates releasing the charged molecules. - This absorption mechanism is observed in substances which are highly ionized and maintain their charge at all physiologic pH values. • Endocytosis: It is a cellular process in which substances are brought into the cell. Drug absorbed by endocytosis directly passes into the lymphatic system. The lipid bilayer of the cell membrane has ability to form saccule or vesicle. When the vesicle engulfs a solid particle, the process is known as phagocytosis or cell eating. Particulate matter such as parasite eggs, starch, hair and plastic fragments may enter the circulation by this pathway. When the material engulfed by the vesicle is fluid, it is known as pinocytosis or cell drinking. Oral polio vaccine, botulinum toxin and many allergens are absorbed by pinocytosis. MCQs based on blog 1 1. All are characteristics of passive diffusion, except ______. (a) Drugs moves down the concentration gradient (b) It is an energy independent process (c) Drugs moves up the concentration gradient (d) It is non-saturable process 2. In carrier mediated transport energy is derived from ______. (a) Hydrolysis of ATP (b) Protein metabolism (c) Concentration gradient (d) All of the above 3. The main mechanism of most drugs absorption in GI tract is ______. (a) Active transport (carrier-mediated diffusion) (b) Filtration (aqueous diffusion) (c) Endocytosis and exocytosis (d) Passive diffusion (lipid diffusion) 4. General term having to do with actions of the body on the drug _____. (a) Pharmacodynamics (b) Pharmacogenetics (c) Pharmacokinetics (d) None of these 5. The passage of unchanged form of the drug into the systemic circulation is _____. (a) Absorption (b) Distribution (c) Metabolism (d) Bioavailability 6. Which of the following is carrier mediated transport system? (a) passive diffusion (b) facilitated passive diffusion (c) pore transport (d) endocytosis 7. ______types of drugs are absorbed by pore transport mechanism. (a) Macromolecules (b) Ionic drugs (c) Drugs with molecular weight 100-400 (d) Water soluble drugs of molecular weight less than 100 8. If the given drug is absorbed by passive diffusion what will be its absorption kinetics? (a) Zero order (b) First order (c) Second order (d) Pseudo-zero order Check your answers below:


Read the notice carefully. Exam is NOT CANCELED.

Essential Pharmacy Review for Drugs Inspector Exams: Featuring the Latest Updates For Pan-India Drugs Inspector Exams and GPAT- In the dynamic field of pharmacy, the role of drugs inspectors has never been more critical. As the guardians of public health, drugs inspectors ensure that pharmaceuticals meet the highest standards of safety, efficacy, and quality. Preparing for the drugs inspector exams requires a solid understanding of complex topics, combined with the ability to apply that knowledge effectively. If you are preparing for the drug inspector exams, one essential resource to consider is the book, "Essential Pharmacy Review for Drugs Inspector Exams". This comprehensive guide is designed to equip aspiring drug inspectors with the necessary tools to succeed.
Diploma in Pharmacy Exit Examination (DPEE) will be conducted as per gazette notification of Pharmacy council of India dated 24th February, 2022 to declare a Diploma in Pharmacy holder eligible for enrollment and practice as a registered pharmacist. An exit examination for the registration of a Diploma in Pharmacy holder is a good move as it will improve the quality of pharmacist which will lead to better community pharmacy services. It will boost the self confidence in pharmacy students. This exam will encourage students to put effort into their learning. Execution of exit exams in India definitely will revamp the pharmacy profession.

It is a dream of many diploma holder and graduate registered pharmacists to enter into the Government Services as a pharmacist to serve the nation. As the posts for Govt. pharmacist are limited in comparison to the availability of registered pharmacists in India, there is a huge competition among the pharmacists for these posts. So Govt. agencies conduct recruitment examinations and interviews to select the best candidate for these posts.
